
House Call Doctor Visits Make Life Easier for Seniors and Caregivers

Important: This is an informational article to explain how house call doctor visits can benefit seniors. DailyCaring isn’t a medical organization, we aren’t medical professionals, and we aren’t affiliated with any healthcare organizations. We aren’t qualified to respond to any medical questions.
House call doctor visits benefit older adults and caregivers
Getting your older adult to the doctor’s office for an appointment can be difficult or sometimes impossible.
Whether they’re frail, can’t walk on their own, or have Alzheimer’s or dementia , getting out of the house is hard on both of you. Going to a doctor’s office can also expose seniors to germs or harsh weather.
We explain what a house call doctor is, what type of insurance they accept, how to find one, and what to look for in terms of services.
What is a house call doctor?
Today, many doctors are bringing back the old practice of visiting patients in their homes. With house calls, older adults don’t have to go through the stress and difficulty of getting to the doctor’s office. And neither do you.
Another bonus is that these doctors usually spend more time with patients. You won’t have to fit all your questions into a 15 minute visit.
Do they accept Medicare?
Yes, many house call doctors accept Medicare , private insurance, and sometimes Medicaid . It usually costs the same as a regular office visit.
But every house call doctor is different, so make sure you understand their fees and accepted insurance plans before making an appointment.
How to find a house call doctor
Some large health care systems like Kaiser Permanente or the VA have programs that include home visits by doctors and nurses. For example, Kaiser’s home-based palliative care program includes house calls.
Even your older adult isn’t part of a large health network, it’s worthwhile to ask your older adult’s doctor if they have home doctor visit programs.
The American Academy of Home Care Medicine’s provider directory is another way to locate a house call doctor in your area.
You can also use Google to search for “house call doctor” + your city or county or “home doctor visit” + your city or county (don’t include the quotation marks).
What to look for in a house call doctor
Before booking an appointment, make sure you understand the doctor’s services, fees, and billing.
Questions to ask:
- Do you specialize in treating seniors, people with Alzheimer’s or dementia , or those with multiple chronic conditions ?
- Do you accept Medicare , Medicaid , or my older adult’s private insurance plan?
- If we want, can we also keep my older adult’s primary care doctor?
- Will you communicate with my older adult’s existing doctors and specialists so their care is coordinated?
Examples of house call doctor private practices
We want to be clear that we’re not recommending any specific home doctor services or companies and aren’t affiliated with any of these businesses. These are examples to give you an idea of what a house call doctor looks like and the type of services that are typically offered.
Examples of what a house call doctor looks like:
- Visiting Physicians Association (VPA)
- Bay Area House Call Physicians
- Kindred House Calls
Recommended for you:
- 4 Expert Tips for Managing Multiple Chronic Health Conditions in Seniors
- 7 Tips for Helping Seniors at the Doctor: Being a Health Advocate
- Should Seniors See a Geriatrician?
By DailyCaring Editorial Team Image: Now It Counts
This article wasn’t sponsored and doesn’t contain affiliate links. For more information, see How We Make Money .
- Share Article on:
Related Articles

Prevent Falls with 5 Warning Signs of Mobility Issues in Seniors

4 Great Sources of Tasty Low Sodium Recipes for Seniors

5 Questions to Ask Doctors About Tests and Treatments for Seniors

4 Common Eye Diseases That Cause Blindness in Aging Eyes
18 comments, tony carrancho.
My parent s lives in [redacted for privacy]. How do i get started locating a house call doctor. I am pretty sure there insurance covers this. Thank you. TONY
DailyCaring
We hope the tips and suggestions in the article above will help you find a house call doctor in your parents’ local area.
Susan Quercio
My 95 year old father has a deep cough and he is disoriented. Temp 99 degrees.
Please contact your father’s doctor immediately or the local hospital to find out how to safely get him examined by a doctor (to reduce risk of exposure to Covid-19).
DailyCaring isn’t a medical organization, we aren’t medical professionals, and we aren’t affiliated with any healthcare organizations.
Ruby m VanNostern
I live in [redacted for privacy] and need a doctor visit in home.
This article includes suggestions for how you can find house call doctor services in your area. At DailyCaring, we aren’t doctors and don’t provide any medical services. We hope you’re able to find a great house call doctor in your area.
Stewart Goldman
need Doctor for a home visit Andrews N.C.
Joseph Artusa
I need a doctor
Linda Williams
I was released from the hospital on Thursday after 5 days.I am not able to go to Dr office but most definitely need to be checked.Still having breaking problems and am very week.I have severe asthma and blood pressure was running very high from so much steroids.Could I possibly get help.Thanks so much.
I’m so sorry to hear that you’re not feeling well. Since you’re noticing some issues with your recovery, it’s essential to call your primary doctor immediately. Since they’re the ones who have been treating you and are familiar with your recent hospitalization, they’re the best people to advise you on what you need. If you need help getting to your doctor’s office, you may want to contact your local Area Agency on Aging or a ride sharing service. Or, use the tips in this article to search for a doctor in your area who makes house calls.
Here are some articles that may be helpful: — 8 Ridesharing Services for Seniors https://dailycaring.com/8-ridesharing-services-for-seniors/ — 6 Affordable Senior Transportation Options https://dailycaring.com/6-affordable-senior-transportation-options/ — Local Community Resources for Seniors and Caregivers: Area Agency on Aging (to connect you with local organizations that may be able to help) https://dailycaring.com/local-community-resources-for-seniors-and-caregivers-area-agency-on-aging/ — 4 Ways to Know If Seniors Need to Return to the Hospital https://dailycaring.com/4-ways-to-know-if-seniors-need-to-return-to-the-hospital/
(DailyCaring doesn’t provide any services and isn’t affiliated with any medical providers.)
What areas do you service?
This article explains that house call doctor services are available and could help senior and caregivers. We also share suggestions for finding one in your area, but we do not provide any services ourselves. I hope you’re able to find a great local house call doctor!
What areas do you service
This article includes suggestions for finding house call doctor services in your area. We at DailyCaring aren’t doctors and don’t provide any medical services. I hope you’re able to find a great house call doctor in your area.
need a home care doctor
I hope the information above helps you find a great home care doctor in your area.
Leave a Reply Click here to cancel reply.
Cancel reply.
- Healthcare Services
- Find a Doctor
- Patient Portal
- Research and Education

Your recent searches
- Find a Location
- Nursing Careers
- Physical Therapy Careers
- Medical Education
- Research & Innovation
- Pay My Bill
- Billing & Insurance Questions
- For Healthcare Professionals
- News & Publications
- Classes & Events
- Philanthropy
House Call Program - MedStar Total Elder Care
Browse this page
Promoting the health and dignity of frail elders
Many elders struggle with disability and severe chronic illness and have difficulty getting to the doctor’s office. As a result, their health may suffer and lead to unnecessary ER visits, hospitalization, or nursing home care. In 1999, recognizing the needs of such elders and their families, we created the MedStar House Call program - MedStar Total Elder Care to provide full medical and social services that help elders remain in their homes with dignity. These teams now serve both Washington, D.C., and Baltimore, MD.
The MedStar House Call Program - MedStar Total Elder Care is nationally recognized for the quality and outcomes of our care. We serve patients at home with a team of geriatricians, nurse practitioners (NPs), social workers, office nurses, and coordinators. We make routine and urgent house calls (in-person or via telehealth with video or audio-only phone visits). Our medical staff is also available by phone 24/7 for urgent issues. We provide access to state-of-the-art hospital and specialty care. Additionally, our physician team follows our patients if and when they are admitted to the MedStar Washington Hospital Center.
The House Call program serves our neighbors in Washington, D.C., and Baltimore.
Medstar house call program .
(operating under MedStar Total Elder Care, LLC)

Our program services
Medical house calls and primary care by doctors and nurse practitioners with expertise in the care of older adults
Counseling and caregiver support by social workers and team staff
We offer tests and treatments at-home, and at the hospital as needed
Home delivery of most medications and equipment
Coordination of specialist care at MedStar Washington or MedStar Good Samaritan
Coordination of home nursing, rehab therapy, and hospice
Coordination of support services such as home aides and legal assistance
On-call physicians: 24 hours a day, 7 days a week (by phone)
Mobile electronic health record (EHR)
D.C. Neighborhood only – Case management for Medicaid Elderly Persons with Disabilities (EPD) Waiver
Hospital care and specialists
Our team coordinates emergency, hospital, and specialty care at MedStar Washington and MedStar Good Samaritan. Patients may keep their previous specialist doctors; we work with them as needed. We refer to MedStar Good Samaritan, MedStar Washington, for home-based podiatry or other new specialist care. If House Call patients require hospitalization, and 911 is not needed, our team can arrange transportation and admission to MedStar Good Samaritan or MedStar Washington when beds are available.
Social work services
Our dedicated team of social workers provides:
Psychosocial assessment
Care Coordination
Development of an individual treatment plan
Information and referral to community resources and supports
Caregiver education, support, and counseling
Advocacy to connect with other service networks and legal counseling
Crisis intervention
Assistance with identifying alternative living arrangements, as needed
Eligibility
Enrollment and insurance.
To qualify for the MedStar House Call Program, patients must:
Be 65 years or older and have difficulty getting to the doctor’s office
Have Medicare, Medicaid, or another participating insurance plan
Stop seeing their previous primary doctor and agree to have us take on that role following the first visit
Live in a qualifying ZIP code
Our office is open 8:30 a.m. to 4:30 p.m., Monday - Friday.
When calling about new patient enrollment, please have the following information:
Patient's name, address, telephone number
Patient's date of birth and social security number
Patient's next of kin and emergency contact information
Patient's health insurance information (including type and group number)
Patient's current medical conditions and concerns
Ability to retrieve patient's recent medical records
Baltimore neighbors, print and complete our Intake Questionnaire form
As in most doctor's offices, your main health insurance (such as Medicare) covers 80 percent of House Call visit fees, and any secondary insurance covers the other 20 percent. The patients who do not have any secondary insurance are responsible for the 20 percent co-pay.
Qualifying ZIP codes
View the map below to check if you live in a qualifying ZIP code. Call our Washington, D.C., or Baltimore location to confirm MedStar House Call Program eligibility at your exact address.
Washington, D.C.,
View our brochures
Baltimore region brochure
Washington, D.C., region brochure
Washington, D.C., region team - 202-877-0570
Physicians Eric De Jonge, MD, – Section Director Guy (Binny) Chang, MD Nurse Practitioners Nancy Sassa, CRNP - Chief Alexandra (Caitlin) Geary, CRNP Michelle Sullivan, CRNP Office Nurse Kendel Ogbeab, RN Social Workers Gretchen Nordstrom, LICSW - Chief Kellie Jones, LICSW Ruth Shea, LICSW Operations Manager Isi Koroma Care Coordinators LaWanda Holeman Sandra Mills Carrie Carmon Yvette Williams
Baltimore region team – 443-444-6100
Physicians George Taler, MD Sharareh Badri, MD Nurse Practitioner Dorothy Were, CRNP Adama Panda, CRNP Nurse Nerland Dimanche, RN, MSN Social Worker Marina Nellius, LMSW Operations Director Shereen Greene, MBA Care Coordinator Taurshica Lee
Operational support
Executive Director George Hennawai, MD AVP Operations Julie Beecher, MS, MPH
Baltimore Neighborhood
To learn more about our services in the Baltimore region, call us today.at 443-444-6100.
Washington, D.C., Neighborhood
To learn more about our services in the Washington, D.C., region, call us today at 202-877-0570
Related services
Senior Home Care: Services, Costs and Tips for Aging in Place
Learn about in-home caregiving options for seniors who want to stay in their houses for as long as possible.
This article is based on reporting that features expert sources.
What Is Senior Home Care?
Aging is a fact of life. We simply can’t stop the clock, and for most adults, there will come a time when a little extra assistance performing the tasks of daily living would be helpful.

Getty Images
In fact, someone who turns 65 today has a nearly 70% chance of needing some type of long-term care in their remaining years, according to the Department of Health and Human Services.
For some people, this support means moving into an assisted living community or a nursing home. For others, aging in place is a much more attractive goal.
What Is Aging in Place?
"Aging in place" is exactly as it sounds: Spending your twilight years in your home, without having to move to a senior care facility.
It's also a popular choice. According to AARP's 2021 Home and Community Preferences Survey, 77% of adults age 50 and older want to stay in their homes for the long term. Only 29% of survey respondents said they plan to relocate to another community as they age.
What's key to staying in your familiar environment is senior home care .
“Senior home care allows seniors to continue living as independently as possible at home, with limited care provided as the individual’s needs require,” says Bob Rees, chief sales officer with eHealth Inc., a health insurance broker and online resource provider headquartered in Santa Clara, California.
Senior Home Care vs. Senior Home Health Care
Support for aging in place can take a variety of forms – from technology to human services – but it tends to take two primary forms: senior home care and senior home health care.
Senior home care
This category involves personal care assistance , such as light housekeeping and running errands.
“Maybe they help someone get dressed or take a shower,” notes Danielle Pierotti, clinical associate professor and director of undergraduate studies with the School of Nursing at Idaho State University in Pocatello.
These caregivers are not usually licensed to provide health care services, and the training they receive varies from company to company. This form of care is also typically paid for out of pocket by the senior or the family.
Senior home health care
This category of care, which can include both medical and personal care components, involves a licensed professional, such as a registered nurse or a physical therapist, and a physician's orders, Pierotti says. Senior home care, on the other hand, may not involve a physician.
Home health care services are also usually covered by Medicare or a private insurer.
To qualify for Medicare coverage , you’re may be required to be homebound.
Home health services that may be covered by Medicare include:
- Skilled nursing care.
- Physical or occupational therapy.
- Speech-language pathology services.
- Injectable osteoporosis drugs for women.
- Durable medical equipment and other medical supplies for home use.
“Before coverage kicks in, you generally need to be seen face-to-face by a doctor to certify that you are in need of home health care services,” Rees adds.
What Senior Home Care Services Are Available to Help You Age in Place?
The menu of options offered by senior home care organizations is virtually limitless, but it's often dictated by the family budget. Services for seniors receiving in-home care may include:
- Light housekeeping, such as cleaning and laundry services.
- Meal preparation or delivery and diet monitoring.
- Assistance with eating.
- Personal services, such as assistance with bathing, dressing or walking.
- Assistance with shopping and other errands.
- Companionship and social interaction.
- Transportation.
- Volunteer services, which can run the gamut from simple companionship to transportation, personal care, emotional support and more specialized skills, such as assisting with paperwork or other needs.
Senior home health care services, on the other hand, can include:
- In-home nursing care, such as wound dressing, IV therapy, health monitoring, pain control and other nursing duties.
- In-home physical, occupational or speech therapy, as mentioned.
- In-home doctors' visits or telemedicine checkups via video conferencing or phone.
- Medical social services, such as counseling and identifying community support and other resources.
- Medication management or reminders.
Types of In-Home Senior Caregivers
Different organizations offer these services using one of three models, says Lakelyn Eichenberger, gerontologist and caregiver advocate for Home Instead Inc., a network of independently owned and operated senior home care agencies headquartered in Omaha, Nebraska.
Independent caregivers
This type may be a more casual arrangement, and the care may be coming from a friend, family member or a local provider that you hire independently.
Small caregiver registries
In some cases, a local organization or registry connects families with caregivers who are available. This is also a form of independent caregiving that the family would pay for out of pocket, but it may be a more formalized arrangement between the senior and the caregiver.
Agency caregivers
With this model, an agency employs professional caregivers who are sent into clients’ homes to care for them. Agencies can range in size from local mom-and-pop operations to regional or national franchise organizations. Some of these agencies may work with insurance companies to handle billing for what can be covered by Medicare, but it depends on how the business operates.
Some agencies also offer specialized memory care services for older adults who want to remain in their home but are dealing with cognitive decline, dementia or Alzheimer’s disease. Senior health caregivers offering these types of services are typically trained in what to watch out for and what to do when the individual’s health starts to change.
Other options
Creative living and care situations are also popping up.
“What we’re starting to see as the baby boomer generation grows older are a number of other options, including tiny house communities that offer independent living with some aspects of daily life being communal – think group meal time,” says Dr. Elizabeth Landsverk, a geriatrician based in the San Francisco area.
For example, she continues, some “retirees have chosen to live on a boat – I am one of them – as long as they are fit and have someone else on hand to help. We’re also hearing more and more about some who choose to live aboard cruise ships as most day-to-day needs like meal preparation, laundry, etc. are included in the cost.”
When Do You Need Senior Home Health Care?
Seniors usually need short-term assistance in situations such as:
- After coming home from a hospital stay .
- While recovering from an illness or injury.
- While experiencing chronic conditions, advanced age or cognitive decline .
In-Home Senior Care Cost
Estimating how much in-home senior care will cost can be challenging: The various combinations of services, plus the level of care needed and geographic location, all factor into price.
“The cost of care in a city like San Francisco tends to be higher than Omaha, Nebraska,” Eichenberger points out.
Generally, however, the median annual cost for homemaker services is $59,488, or $26 per hour, according to Genworth Financial's 2021 Cost of Care Survey (the most recent data available). The median annual cost for a home health aide is $61,776, or $27 per hour.
Most in-home care companies charge by the hour, with a typical range between $20 and $40, depending on the market. Each organization also has its own fee structure and cost ranges.
“Sometimes people think that home care is more expensive than it really is, but then they’ll underestimate the cost of a nursing home . Oftentimes, depending on the level of need , the opposite is true,” Eichenberger says.
For instance, the annual median cost of a semi-private room in a nursing home is $94,900, according to the Genworth survey. A private room in a nursing home is $108,408, about twice the median of in-home care.
“Having care at home can delay the need to move to a facility or community setting in a lot of cases,” which may cut down on lifetime cost, Eichenberger notes.
Ways to Pay for Senior Home Caregiving
For the most part, home care is covered out of pocket by families, though some long-term care insurance options may cover these fees.
In addition, Medicare Advantage benefits, as of 2019, include non-skilled home care services, such as assistance with tasks like bathing and dressing.
For both options, check your plan for details.
Is In-Home Senior Care Tax Deductible?
You may be able to deduct some aspects of in-home senior care when filing your taxes. Generally speaking, the medical expenses piece of in-home senior care is tax deductible if these expenses are deemed medically necessary by a physician. These expenses only become tax-deductible once they’ve exceeded more than 7.5% of your adjusted gross income.
For instance, assistance with certain activities of daily living, such as bathing, dressing, eating and toileting, may be deductible if they’re medically necessary and rendered for a minimum of 90 days. Other services, such as companionship or assistance with tasks that have not been deemed medically necessary, would not be tax deductible.
Before deducting any costs associated with in-home senior care services, seek the advice of a certified tax professional for specific guidance.
How to Find the Right In-Home Senior Caregiver
When considering whether elderly home care is right for your situation, Pierotti recommends “being very honest with yourself about what you’re comfortable with and what you’re seeking.” She likens the search for the right mix of services to completing a home renovation project.
“If you think about it in terms of how you would work with any contractor coming into your home – are you the type of person who’s comfortable hiring the plumber, the electrician and the lawn person all by yourself? Or do you want to hire a contractor who’s going to manage all those people? It’s a similar sort of situation,” she explains.
This can be a confusing and difficult aspect of finding the right solution, which is further compounded by the services a senior needs likely changing over time. Aging is dynamic, and it’s hard to predict exactly what assistance will be needed at a given point.
To get started, however, consider taking these steps:
- Talk to your physician about your care needs.
- Outline your budget.
- Research the options in your area.
- Ask lots of questions. Not only can you ask others for referrals to agencies, registries or individuals, but you should also interview multiple caregivers to ensure you're getting the services you need.
Tips for Aging in Place
Aging in place requires an honest assessment of needs versus wants and separating the ideal from reality, Pierotti says.
“‘What I really need is someone to make sure Dad gets a shower twice a week, but what I’d really love is someone who comes in every day and makes sure he has lunch and is dressed,’" she notes. "And then you can begin to break down and think through the things you really want compared to the things that you’d love to have and process those decisions along the way. What are you comfortable with? What can you afford? Where can you get people?”
Other tips include:
- Conducting a home safety assessment. Making modifications to the home may allow you or your loved one to remain there without risk of injury.
- Observing how potential caregivers interact with you or your loved one.
- Making sure that the caregiver is bonded and insured.
- Working with an established agency. If a caregiver is a no-show, the agency will find a replacement for you, Landsverk points out. If you hire on your own, you'll need to find a replacement yourself.
Bottom Line
Pierotti says many people can avoid moving to a nursing home when the right mix of family and community support is identified and employed. But this situation can be challenging for the family caregiver who’s tasked with coordinating care.
“The key thing is that we’re all in this together. As a national community, we’re going to have to talk about aging and what does it mean for all of us,” Pierotti says, adding, “To me, that’s what the conversation about aging is about.”
Having those conversations early and frequently is important to finding the right solution for your family.
The U.S. News Health team delivers accurate information about health, nutrition and fitness, as well as in-depth medical condition guides. All of our stories rely on multiple, independent sources and experts in the field, such as medical doctors and licensed nutritionists. To learn more about how we keep our content accurate and trustworthy, read our editorial guidelines .
Eichenberger is a gerontologist and caregiving advocate for Home Instead Inc., a network of independently owned and operated senior home care agencies headquartered in Omaha, Nebraska.
Landsverk is a San Francisco area-based geriatrician offering an online telemedicine, education and support resource for eldercare professionals, caregivers and families. She is the author of “Living in the Moment: Overcoming Challenges and Finding Moments of Joy in Alzheimer’s Disease and Other Dementias.”
Pierotti is clinical associate professor and director of undergraduate studies with the School of Nursing at Idaho State University in Pocatello. She previously served as president and CEO of ElevatingHOME and the Visiting Nurses Associations of America.
Rees is chief sales officer with eHealth Inc., a health insurance broker and online resource provider headquartered in Santa Clara, California.
Tags: aging , nursing homes , senior citizens , senior health
Most Popular

Patient Advice

health disclaimer »
Disclaimer and a note about your health ».

Your Health
A guide to nutrition and wellness from the health team at U.S. News & World Report.
You May Also Like
What makes a good doctor.
Paul Wynn April 25, 2024

Americans' Primary Care Experiences
Annika Urban April 24, 2024
Does Medicare Cover Cataract Surgery?
Elaine K. Howley April 24, 2024
RSV Vaccines: Who Should Have One?
Stacey Colino April 22, 2024
Your Guide to Hip Replacement Surgery
Lisa Esposito and Elaine K. Howley April 22, 2024
Find a Primary Care Doctor Near You
Payton Sy April 18, 2024

Streamlined Maternity Services Survey
Jennifer Winston, Ph.D. , Xinyan Zhou and Kaylan Ware April 17, 2024

Major Food Allergens
Claire Wolters April 15, 2024

What to Know About Creatinine Levels
Christine Comizio April 12, 2024

Medicare Coverage for Hearing Aids 2024
Paul Wynn and C.J. Trent-Gurbuz April 12, 2024

House Calls – We Bring the Doctor’s Office to the Patient
At Mobile Physician Services, we provide comprehensive care to improve the health and quality of life of our patients – in the convenience and comfort of their own home. Our team of board-certified doctors, advance nurse practitioners, and physician assistants specialize in providing care for patients with medically complex and chronic conditions.
Our Services
We accept Medicare, many insurance plans, and self-pay.
To find out more about our services:
Call Toll-free: (855) 232-0644
E-mail us at [email protected]
Primary Care
Pain management, palliative care.
At Mobile Physician Services, our customized care teams provide patients with both comfort and familiarity as they work with a dedicated primary care provider and care coordinator to improve their health. Our physicians and staff take a proactive approach to preventive care, chronic disease management, and chronic illness support right where you live.
Each home visit includes an in-depth examination and individualized treatment plan, which is monitored and adjusted through routine follow-up visits. The primary care provider will deliver your ongoing care and will recommend to you specialty services as needed.
- Annual Wellness visits : This wellness visit allows your primary care provider to create or update your personalized prevention plan. This visit includes a review of your medical and social history related to your health and may include counseling about preventive services. This plan may help you to prevent or reduce the chances of future illness based on your current health and risk factors.
- New Illness Exams : When a new symptom or ailment arises, call us. Early indications of not feeling well could be a clue that you may be getting sick. A symptom in one part of the body may also be a sign of a problem in another part of the body. Moreover, unrelated symptoms that might seem minor on their own, could be warning signs of a more serious medical disease or condition. The new illness exam can be very brief or more detailed depending on your concerns and the provider’s findings.
- Follow-up Care: Involves a regular medical checkup, which may include a physical exam and laboratory testing. Follow-up care checks are a proactive way of assessing the potential for and preventing health problems from returning after treatment of a disease has ended or an illness has seemingly passed.
- Referral for Specialty Care : Referrals are the link between primary and specialty care. The referral coordination includes the documentation of patient care activities, the transfer of information, the inter-provider communication itself, and the integration of care services to the patient. Mobile Physician Services is a multi-specialty practice so many of these specialty referral services can be made seamlessly with little inconvenience or disruption to the patient and caregivers regular routines.
- Medication Management: Medication management is a treatment structure that ensures our patients are receiving optimal therapeutic results from their prescription medications, both in the short and long term. Our team’s goal is to mitigate medication noncompliance and monitor all prescriptions treatments so that drug interactions complement one another for the most optimal outcome for our patients.
The provider may be a physician, advanced practice nurse or a physician assistant. A dedicated care coordinator will also be assigned for each patient to help arrange comprehensive services and assist patients and their caregivers.
- Online Patient Portal: You and your designated caregiver, if you choose, will be able to connect with your provider through a convenient, safe and secure environment which allows access to your health records and a way to communicate with our staff in a timely manner.
- Telephone Assistance : On call providers are available 24/7 weekdays and weekends.

Our psychiatry team specializes in the diagnosis and management of mental, emotional and behavioral disorders. They carefully evaluate each patient to develop an individualized treatment plan to improve the patient’s overall mental and physical well-being.
- Depression : Depression is a common and often serious medical illness that negatively affects how you may feel, the way you may think, and how you may act. Depression can cause feelings of sadness, despair and hopelessness, which may lead to a loss of interest in activities you once enjoyed.
- Anxiety : Intense, excessive, and persistent worry and fear about everyday common situations. The worry or anxiety could make you feel fatigued, irritable, and interfere with your regular sleep habits.
- Dementia : An overall term that is used to describes a collection of symptoms related to an individual’s decline in memory or other thinking skills. It may be severe enough to diminish a person’s ability to perform everyday common activities. The effects of dementia can negatively influence your memory, thinking and social abilities.
- Phobias : A phobia is when you experience excessive panicking or an irrational fear reaction to a situation. If you have a phobia, you may experience a deep sense of dread or fright when you encounter the source of your fear. The fear may be a certain place, situation, object, animal or even another person.
- Behavioral disorders : Attention deficit, hyperactivity, bipolar, learning, defiant or conduct disorders are all examples of complaints that may have a detrimental impact on a person’s interpersonal relationships with family, friends, and co-workers.
Our team can provide behavioral counselling and medical therapy, when appropriate, to help a patient feel better about themselves and to assist them with better coping and managing their condition.

Our wound care specialists have been trained in the attention and treatment of all types of acute and chronic wounds. They have skill and experience in wound debridement and wound care procedures – managing chronic, non-healing wounds and infections, with a demonstrated care that fosters healing… right in the patient’s own home.
We specialize in serving homebound patients who may also be bed-bound or have difficulty in walking or moving around. As a result, immobility compression sores develop at pressure points on the body when the weight of an immobilized individual rests continuously on a firm surface, such as a mattress or wheel chair. Often these same patients are on oxygen or have high-risk medical conditions which makes it an even more challenging and stressful effort for them to travel to a doctor’s office for an appointment. Thus, the necessity for in home care and treatment.
Wounds that benefit from specialized wound care techniques include:
- Diabetic foot wounds and ulcers
- Post-surgical wounds
- Traumatic wounds caused by injury
- Arterial and vein stasis caused by lack of circulation
- Immobility pressure sores. (Bed sores from stillness)
We work closely with home health agencies to provide ongoing care and monitoring of patient’s wounds.

Our board-certified podiatrists treat foot pain, wounds, and more. Treatments may include but are not limited to treating conditions of the lower extremities which could hinder mobility.
- We will review each patients’ medical history to evaluate the condition of the feet, ankle or lower leg
- Carry out a diagnosis on the feet and lower legs through examination and medical tests
- Order physical therapy when deemed necessary
- Treat wounds of the lower extremities using various wound care modalities. This may include debridement to improve the healing potential
- Promote prevention, health & well being, the treatment and management of the foot and related problems, disability, deformity, and the pedal complications of chronic diseases for the elderly
- Prescribe and fit prosthetic appliances such as diabetic shoe inserts and evaluate for bracing if necessary
- Refer patients to other specialists for treatment, including conditions such as diabetes or arthritis
- Advise patients on ways to prevent future leg problems and increase speed of recovery
- Monitor the recovery progress of patients to determine the need for change in treatment

We know it’s not always easy to leave home to get the care you need for your eyes. Our optometrists bring state-of-the-art diagnostic eye equipment and technology to your home – making it much easier for you to get the vision care you need.
During a visit, your doctor will exam each eye for signs of serious issues such as glaucoma, cataracts, macular degeneration, and detached retinas, among other conditions.
Receiving regular eye exams regardless of the state of your vision can help detect serious eye problems at their earliest stages ─ when they are most treatable. During an eye exam, your doctor will observe and evaluate the health and condition of the blood vessels in your retina, which can be good indicators of the health of your blood vessels throughout the rest of your body.
- Comprehensive eye exams : This exam goes beyond a simple vision screening. A comprehensive eye exam includes a host of tests in order to do a complete evaluation of the health of your eyes and your vision.
- Annual retina exams : A retinal exam allows your doctor to evaluate the back of your eye, including the retina, the optic disk and the underlying layer of blood vessels that supply the retina.
- Eyeglass fittings : A prescription works best when your eyeglasses are properly fitted. Improper fitting may cause pinching, distorted vision, headaches, and even dizziness. Our doctors will make sure your prescription lenses and frames are working together for you.
- Diabetic eye exams : Diabetes does not have to lead to vision loss. Taking an active role in managing your diabetes can go a long way in curbing later complications. Regular eye exams, good management of your blood sugar and blood pressure, along with early intervention for vision problems can help prevent vision loss caused by diabetic retinopathy. Retinopathy is caused by damage to the blood vessels of the light-sensitive tissue at the back of your eye.
- Refractions: This test is given as part of your routine eye examination. It is often referred to as a vision test. This test assists your eye doctor in measuring you for the exact lens prescription you will need.
- Eye injuries: Eye trauma could be the result of a sudden blow to the eye. It may cause the eye to suddenly compress and retract which could cause damage to your eye and the surrounding tissue. Even if the injury may seem minor, all eye injuries should be furthered examined by a doctor for possible more serious and underlying injuries.
- Eye infections: The most common eye infection is conjunctivitis, also known as pink-eye. An eye infection can happen in almost any part of your eye, including your eye lid, cornea and optic nerve. Symptoms of eye infections may include redness, itching, swelling, discharge, pain, or problems with vision. Always consult with your doctor before treating, as recommended actions are contingent on the cause of the infection.
- Low-vision exams: A low vision exam is different from a normal eye exam. This functional-vision assessment determines how specific visual impairments affects your ability to perform everyday activities. The exam’s results assist your doctor in prescribing management tools and medications to better enhance and manage your remaining vision.

Pain management is the process of providing medical care that alleviates or reduces pain. Pain management is a subspecialty of general medicine employing an interdisciplinary approach to ease the suffering and improve the quality of life of those living with chronic pain by using a combination of pain medications, joint and muscles injections, and physical therapy techniques.
A pain management specialist is a provider with advanced training in diagnosing and treating pain. Our pain management specialists treat pain stemming from a variety of different causes, whether it’s neuropathic pain or headache, or the result of injury, a surgical procedure, cancer or another illness.

Palliative care is an approach to the holistic care of patients, including family and caregivers, to improve the quality of their lives after the diagnosis of a chronic debilitating disease or life-limiting illness that may cause a host of complaints.
Palliative care can begin at diagnosis and continue to be offered while the patient is continuing active treatment through different phases of their life limiting condition. Palliative care is for any patient with a chronic illness who is experiencing a decreased quality of life because of symptoms related to their illness or treatment, like renal dialysis, oxygen therapy or chemotherapy. The care is provided by a specially-trained team of doctors, nurse practitioners, physician assistants, and other specialists who work together to provide an extra layer of support to the patient and their caregivers.
Palliative care can help in symptom control including not only pain, but nausea, weakness, shortness of breath, fatigue and weight loss at any time during their diseases, not only at the end of life.

Adult Day Care Services
Senior housing options, independent living for seniors, assisted living facilities, a guide to nursing homes.
- Respite Care: What it is and Where to Find it
Family Caregiving: Help and Support for Caregivers
- Online Therapy: Is it Right for You?
- Mental Health
- Health & Wellness
- Children & Family
- Relationships
Are you or someone you know in crisis?
- Bipolar Disorder
- Eating Disorders
- Grief & Loss
- Personality Disorders
- PTSD & Trauma
- Schizophrenia
- Therapy & Medication
- Exercise & Fitness
- Healthy Eating
- Well-being & Happiness
- Weight Loss
- Work & Career
- Illness & Disability
- Heart Health
- Childhood Issues
- Learning Disabilities
- Family Caregiving
- Teen Issues
- Communication
- Emotional Intelligence
- Love & Friendship
- Domestic Abuse
- Healthy Aging
- Aging Issues
- Alzheimer’s Disease & Dementia
- Senior Housing
- End of Life
- Meet Our Team
What is aging in place?
Home care services to help you age in place, is aging in place right for you, aging in place vs. other types of senior housing, coping with changes in your independence, finding home care services, talking to a loved one about home care services, home care services for seniors: aging in place.
Want to age in place? Learn about the many home care services that can help you stay in your own home and maintain your independence as you get older.

Aging in place means staying in the comfort of your own home for as long as possible as you get older, rather than moving into a retirement or long-term care facility. Aging in place may be a viable option if you only need minor assistance with your daily activities, enjoy a close network of family and friends nearby, and can utilize the right home care services to cover your needs.
By exploring the range of services available, you can decide if aging in place is the best way for you to maintain your independence and make the most of your golden years.
While it may be hard to accept, most of us will require some type of care assistance after the age of 65. You may be used to handling everything yourself, dividing up duties with your spouse, or relying on family members for minor help around the home. But as you get older and your circumstances change, getting around and taking care of yourself can become more and more difficult.
If the idea of moving to a retirement community, assisted living facility, or nursing home doesn’t appeal, home care services may be able to help keep you living in your own home for longer.
Home care services include:
Household maintenance. Keeping a household running smoothly takes a lot of work. If you’re finding it hard to keep up, you can look into laundry, shopping, gardening, housekeeping, and handyman services. If you’re having trouble staying on top of bills and appointments, financial and healthcare management may also be helpful.
Transportation. Transportation is a key issue for older adults. Maybe you’re finding it hard to drive or don’t like to drive at night. Having access to trains, buses, rideshare apps, reduced fare taxis, and senior transportation services can help prolong your independence and maintain your social network.
Home modifications. If your mobility is becoming limited, home modifications can go a long way towards keeping your existing residence comfortable and accessible. Modifications can include things such as grab bars in the shower, ramps to avoid or minimize the use of stairs, or even installing a new bathroom on the ground floor.
Personal care. Help with the activities of daily living, such as dressing, bathing, or meal preparation, is called personal or custodial care. Home health aides can provide personal care services that range from a few hours a day to around-the-clock live-in care. They may also provide limited assistance with things such as taking blood pressure or offering medication reminders.
Health care. Some healthcare services can be provided at home by trained professionals, such as occupational therapists, social workers, or home health nurses. Check with your insurance or health service to see what kind of coverage is available, although you may have to cover some cost out of pocket. Hospice care can also be provided at home.
Day programs. Day programs or adult daycare can help you keep busy with activities and socialization during the day, while providing a break for your caregivers. Some daycare programs are primarily social, while others provide limited health services or specialize in disorders such as early stage Alzheimer’s.
It’s natural to want to stay at home as you grow older. The familiar can be comforting as we face the losses that inevitably come with aging, and your home is likely filled with fond memories and your neighborhood with familiar people. However, taking a step back to look at the big picture can help you decide whether staying at home for the long term truly is the right step for you.
Too often, decisions to leave home are made abruptly after a sudden loss or health crisis, making adjustments all the more painful and difficult. Earlier planning and examining which home care services are available can make it easier to make the choice that’s right for both you and your family.
[Read: Senior Housing Options]
Of course, everyone’s needs vary, depending on factors such as how much support you have, your general health and mobility, and your financial situation. Here are some of the issues to consider when evaluating your aging in place and home care options:
Location and accessibility. Where is your home located? Are you in a rural or suburban area that requires a lot of driving? If you’re in an area with more public transit, is it safe and easily accessible? How much time does it take you to get to services such as shopping or medical appointments? It’s also important to consider proximity to community services and activities.
Home accessibility and maintenance. Is your home easily modified? Does it have a lot of steps or a steep hill to access? Do you have a large yard that needs to be maintained?
Support available. Do you have family and friends nearby? How involved are they? Are they able to provide you the support you need? Many older adults prefer to rely on family to provide help, but as your needs increase, they might not be able to fill in all of the gaps. Caregiving can be physically and emotionally exhausting , especially if it is primarily on one person such as a spouse or child. Your relationships may be healthier if you are open to the idea of getting help from more than one source.
Isolation. If it becomes difficult or impossible for you to leave home without help, isolation can rapidly set in. You may not be able to participate in hobbies you once loved, stay involved in community service that kept you motivated, or visit with friends and family. Losing these connections and support is a recipe for depression.
Medical conditions. No one can predict the future. However, if you or your spouse has a chronic medical condition that is expected to worsen over time, it’s especially important to think about how you will handle health and mobility problems. What are common complications of your condition, and how will you handle them?
Finances. Making a budget with anticipated expenses can help you weigh the pros and cons of your situation. Alternate arrangements like assisted living can be expensive, but extensive in-home help can rapidly become expensive as well, especially at higher levels of care and live-in or 24-hour coverage.
Your family’s opinions . Naturally, you have the final decision as to where you want to live, but input from family members can be helpful. Are they worried about your safety or a health problem that will eventually require heavy care? Listening to concerns and keeping an open mind are key.
If you feel overwhelmed by the upkeep of your home, cut off from social amenities, or simply want more companionship with others your age, an independent living or retirement community may be a better option.
The housing is friendlier to aging adults and while residents live independently, most communities offer amenities and services. As the name suggests, independent living is more about making life easier rather than a loss of independence.
If you or your spouse have a lot of medical needs, though, you may be better off considering an assisted living facility or nursing home . For more information, read Senior Housing Options .
Speak to a Licensed Therapist
BetterHelp is an online therapy service that matches you to licensed, accredited therapists who can help with depression, anxiety, relationships, and more. Take the assessment and get matched with a therapist in as little as 48 hours.
It’s normal to feel confused, vulnerable, or even angry when you realize you can’t do the things you used to be able to do. You may feel guilty at the prospect of having to rely on outsiders to do things you’ve been used to doing for yourself. Or you may feel uncomfortable about having “strangers” in your home. By acknowledging these feelings and keeping your mind open to new ways to make life easier, you’ll not only cope with your change in situation better but may also be able to prolong other aspects of your independence for longer.
[Read: Aging Well]
Be patient with yourself. Losses are a normal part of aging and losing some of your independence is not a sign of weakness. Allow yourself to feel sad or frustrated about changes in your home care situation without beating yourself up or labeling yourself a failure.
Be open to new possibilities. Your loved ones may offer suggestions about home care services to make your life easier. Rather than dismissing them out of hand, try to keep an open mind and discuss the options. Sometimes, new experiences and situations can lead to you developing new friendships or discovering new possibilities.
Try a trial run of services. A trial run lets you have the chance to experience the benefits of home care services without having to commit to anything long-term.
Once you’ve figured out your needs, it’s time to evaluate which home care services are right for you and where to find the best providers. Of course, it can be difficult to entrust your home or personal care to others, especially people you don’t know. Whether you engage a home care service provider directly or work through an agency, you can allay your fears by conducting some basic research.
Start by seeking referrals from family, friends, or neighbors. There may be a neighbor who could regularly check-in with you or provide yard maintenance, for example. Local religious groups sometimes offer meals or social activities for older adults. Ask the people you know if they have care providers they can recommend. Your doctor or other healthcare professional may also be able to provide referrals.
Full-service agencies usually come at a higher cost but provide prescreened applicants who have already had background checks. Since the caregiver works for the agency, they take care of billing and tax issues. They may also be bonded for issues such as theft. If a caregiver quits or is not working out, an agency can usually find a replacement quickly, and may also provide coverage if a caregiver calls in sick.
Independent providers usually come at a lower cost, but require more legwork on your part. You’ll need to handle any tax requirements and perform background checks and identity verification. In the case of illness or sudden termination, you’ll also be responsible for finding a replacement provider.
Tips for hiring home care providers
How you go about hiring home care providers will partially depend on what kind of help you are looking for. Hiring someone to handle shopping or yard maintenance, for example, is different from hiring someone to provide hands-on or live-in personal care. However, there are some basic tips to keep in mind. Remember that the more time and homework you spend in the initial hiring process, the better the chances of success.
- Conduct an in-depth interview with each candidate . Screening applicants on the phone should always be followed with an in-person interview.
- Be specific about all of the tasks , skills, and schedules involved and be sure that the person you are considering is comfortable with them all.
- Discuss compensation and payment schedules . Do not pay for services in advance.
- Request several work and personal references , and check them carefully. Verify the information provided, and ask all references about reliability, trustworthiness, punctuality, and the care provider’s ability to handle stress.
- Perform background checks . If you’re working through an agency, these are often provided, but you’ll want to check exactly what is covered. Background checks can be done inexpensively through online agencies and alert you to potentially serious problems.
- If you are working with an agency, make sure you understand what is covered. Are there additional fees that apply to specific services or add-ons? If needed, what are the procedures for termination or requesting another provider?
- Don’t be afraid to move on if it’s not the right fit. It’s important that you feel comfortable with a home care provider who’s delivering services in the privacy of your own home. If you don’t, try talking to the provider to see if any miscommunication can be resolved. If not, don’t be afraid to look for another.
It can be frightening and painful to see someone you love struggling to care for themselves. Perhaps you’ve noticed that your loved one’s home has become much messier than it used to be, or that they are wearing stained, dirty clothes. Maybe it’s clear that they haven’t had a bath for a while, or when you open the refrigerator, there’s hardly any food inside. Or perhaps your loved one has suffered a recent fall or you’ve seen a pan burning unattended on the stove.
Sometimes, declines can happen gradually or a sudden change in health or a significant loss can trigger problems. Whatever the reason, if you’re worried about a loved one’s safety or the condition of their home, it’s important to broach the subject carefully.
Express your concerns as your own, without accusing. An older loved one might be more open to your honest expressions of concern. For example, instead of saying “It’s clear you can’t take care of yourself anymore. Something needs to be done,” try “I’ve really been worried about you. It hurts me to think that you might not be getting everything you need. What do you think we should do?”
Respect your loved one’s autonomy and involve them in decisions. Unless your loved one is incapacitated, the final decision about care is up to them. You can help by offering suggestions and ideas for home care services. If you’re worried that home care might not be enough, what other options are available? You can frame it as something to try temporarily instead of trying to impose a permanent solution.
Try to find the real reasons behind any resistance. A loved one who’s resistant to receiving help could be frightened that they are no longer able to do tasks that were formerly so easy. It might be more comfortable to deny it and minimize any problems. Perhaps they’re grieving the loss of a loved one, or frustrated at not being able to connect with friends as easily as they once did. Or maybe they’re uncomfortable with the idea of having outsiders in their home.
Enlist the help of others. Does your loved one know others who have used home care services? Talking to others who have had positive experiences can sometimes help remove fear of the unknown. Sometimes hearing feedback from an unbiased third party, such as a doctor or geriatric care manager, can help a loved one realize that things need to change.
Helplines and support
Home care services.
Eldercare Locator – A national searchable database of community resources for elder care, from transportation to meals and home care. You can also call 1-800-677-1116. (US Department of Health and Human Services)
Help at Home – A guide to understanding how to get care and support for seniors in the UK. Or call 0800 055 6112. (Age UK)
Aged Care Information – Information on contacts and services, including home care services for seniors. Or call 1800 200 422. (Australian Government Department of Social Services)
Programs and Services for Seniors –Information on services for older adults, including home care services. Or call 1-800-622-6232. (Government of Canada)
Meals on wheels services
Find a Meals on Wheels Provider Near You – A searchable database that allows you to find a Meals on Wheels program in your area of the U.S. (Meals on Wheels Association of America)
Get Meals at Home (Meals on Wheels) – Find out if you qualify to receive meals delivered to your home and access a directory of providers in your area. (Directgov)
Meals on Wheels Australia – Find your local Meals on Wheels service. (Meals on Wheels Australia)
More Information
- Act III: Your Plan for Aging in Place - Guide for aging in place at home. (NAIPC)
- Hiring In-Home Help - Tips on hiring home care providers, including pros and cons of using an agency. (Family Caregiver Alliance)
- Introducing In-Home Care When Your Loved One Says ‘No’ - Tips for family caregivers. (Family Caregiver Alliance)
- Hiring In-Home Help—Family Caregiver Alliance. (n.d.). Retrieved July 28, 2022, from Link
- Home Care Services: MedlinePlus. (n.d.). Retrieved July 28, 2022, from Link
- Jones, A. L., & Valverde, R. (2012). Characteristics and Use of Home Health Care by Men and Women Aged 65 and Over. 52, 8. Link
More in Senior Housing
Finding the best center for your needs

Making the best senior living choices for you or a loved one

Choosing the right retirement home or retirement community for you

Tips for choosing a facility and making the transition

Choosing skilled nursing facilities and convalescent homes

Respite Care
Finding respite services for family caregivers

Finding caregiver support and making caregiving more rewarding

Professional therapy, done online
BetterHelp makes starting therapy easy. Take the assessment and get matched with a professional, licensed therapist.
Help us help others
Millions of readers rely on HelpGuide.org for free, evidence-based resources to understand and navigate mental health challenges. Please donate today to help us save, support, and change lives.

- Find Home Care
- What is Home Care
- How Do I Get Started
- Long Distance Care Giving
- How We Assist
- Brochure Library
- Veterans Benefits
- Our Experience
- Our Character
- Home Care Providers
Home Care Services
Companion care, personal care, respite care.
- Fall Prevention
- Life Care Navigation Overview
Palliative Care
- Ready – Set – Go Home
Dementia Care
Alzheimer's care, end of life care.
- Knowledge Center
- Caregiver Jobs
- Media Center
- Franchising
- Why Choose Visiting Angels
- Client Feedback
- Privacy Policy
- Give Us a Review!

How Home Care Works
Learn how "in-home care" can help your loved one and why families across the country have relied on Visiting Angels since 1998 to provide the best senior home care.
- What is Home Care?
- How Do I Get Started?
Types of Care
Our comprehensive services, including companionship, personal care, and specialized services, are designed to keep seniors safe and happy in the comforts of home.
- Ready, Set, Go Home

Discover the Best In-Home Care

Senior Home Care
Visiting Angels is a name families can trust to provide the best home care for their loved ones. We have been a leading elder care provider since 1998. Our professional and dedicated caregivers proudly help older adults live comfortably, independently, and safely in their own homes.
Contact us today to schedule a free in-home assessment and discover why families across America have relied on Visiting Angels for the past 25 years.

Life Care Navigation's customized programs ensures dignified and compassionate care for your loved one so they can remain independent in their home.

Transitional Care

Safe and Steady Fall Prevention Program
Our fall prevention program helps seniors prevent slips, trips, and falls at home. Preventing falls can reduce seniors' risk of hurting themselves. These types of injuries are the number one reason why seniors lose their independence, making fall prevention an important part of aging in place.
Or contact us to learn more.

Our Caregivers

A primary caregiver's role is to ensure loved ones are safe, comfortable, and happy at home. These responsibilities can sometimes be overwhelming, and professional assistance is needed as an extra layer of physical and emotional support. Discover how professional caregivers at Visiting Angels can be a valued extension of your inner circle and help you provide personalized care for your loved ones.
Job Opportunities
Join our team of compassionate caregivers and develop a rewarding career providing seniors with respectful, dignified care in the comforts of their home.
Join our team of compassionate caregivers for a rewarding career providing seniors with dignified care in the comforts of their home.

We are happy to announce the semi-finalists in the running for this year’s Caregiver of the Year Award.
Our commitment.
We believe every senior deserves quality, affordable care and assistance. The Visiting Angels Foundation was established to assist those important organizations that ensure seniors receive the social, medical, educational, and support services they need.

Receive tips and advice on caregiving for your loved one.

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
Effects of home visits on quality of life among older adults: a systematic review protocol
1 Institute for Health Systems Research, National Institutes of Health, Ministry of Health Malaysia, 40170 Shah Alam, Selangor Malaysia
Nurul Salwana Abu Bakar
Ruzimah tumiran, noor hasidah ab rahman, noor areefa ameera mohd ma’amor.
2 Institute of Biological Sciences, Faculty of Science, Universiti Malaya, 50603 Kuala Lumpur, Malaysia
Weng Keong Yau
3 General Medical Department, Hospital Kuala Lumpur, Ministry of Health Malaysia, Jalan Pahang, 50586 Kuala Lumpur, Malaysia
Zalilah Abdullah
Associated data.
Not applicable.
Home visiting services for older adults have been offered for decades to maintain and promote health and independent functioning, thus enhancing quality of life. Previous systematic reviews have provided a mixed picture of the benefits of home visiting programmes in older adults, primarily because of heterogeneity in study designs, targeted populations, and intervention strategies. These reviews may also become out of date; thus, an updated synthesis of relevant studies is warranted. Our objective is to perform a systematic review of recently published primary studies on the effectiveness of multi-professional home visits on quality of life among older adults.
We will perform a comprehensive search for studies investigating the effect of a multi-professional home visit approach on quality of life among older adults. We will conduct the literature search in selected electronic databases and relevant research websites from January 2010 onwards. We will include randomised controlled trials (RCTs), cluster randomised controlled trials (cluster RCTs), and observational studies that enrolled older adults without dementia over 60 years old, along with studies involving multi-professional preventive–promotive home visit approaches not related to recent hospital discharge. We will report our planned review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We will retrieve and record relevant data in a standardised data extraction form and evaluate the quality of the included articles using the Cochrane risk of bias tool and the quality assessment tool for studies with diverse designs (QATSDD). Where appropriate, outcomes will be pooled for meta-analysis using a random-effects model. The main outcomes include quality of life, incidence of falls, depression, dementia, and emergency department admissions.
This review may provide evidence for the effectiveness of home visits in improving older adults’ quality of life. It will potentially benefit health care professionals, policymakers, and researchers by facilitating the design and delivery of interventions related to older generations and improve service delivery in future.
Systematic review registration
PROSPERO CRD42021234531 .
Supplementary Information
The online version contains supplementary material available at 10.1186/s13643-021-01862-8.
Population ageing is a global phenomenon. Most individuals expect to live into their sixties and beyond. The world population of adults aged 60 years and over is expected to nearly double from 12 to 22% between 2015 and 2050 [ 1 ]. In Malaysia, 20% of the total population will be over 65 years old by 2030 [ 2 ]. A recent study indicated that the life expectancy of Malaysian older adults aged 65 years was 79.8 and 82.1 years for males and females, respectively [ 3 ]. Despite the national census statistics defining older adults as those over the age of 65, Malaysia adopted the United Nations’ definition, classifying older adults as those aged 60 years and above for policy development regarding the older adult population [ 4 ]. The older adult population has a multitude of health needs and challenges, along with a deteriorating quality of life (QoL) [ 5 ].
According to the World Health Organization (WHO), QoL refers to “an individual’s perception of life in the context of the culture and value system in which he or she lives and in relation to his or her goals, expectations, standards, and concerns” [ 6 ]. QoL linked to health concepts is defined as the value assigned to the duration of life, modulated by limitations, functional status, perceptions, and social opportunities, which are influenced by diseases, injuries, treatments, and health policies [ 7 ]. QoL is increasingly recognised as a focus for healthcare service delivery in the older adult population. It allows the healthcare providers and policymakers to measure the efficacy of health interventions and evaluate multi-sectoral public policies, which include health, social, community, and policy actions [ 8 ].
Numerous healthcare interventions have been designed and implemented with the goal of maintaining or improving QoL among older adults, and most studies indicate the importance of active ageing. These studies have demonstrated that QoL among older adults can be enhanced through low-cost interventions, such as physical exercise [ 9 – 11 ]. Besides, older adults utilising the home visiting services were shown to have a better QoL outcome [ 12 , 13 ].
Home visits are defined as visits to an individual’s home by professionals, which may include nurses, social workers, physicians, physiotherapists, occupational therapists, pharmacists and other specialists [ 14 ]. There are five types of home visiting services: palliative, rehabilitative, long-term maintenance, therapeutic, and preventive–promotive home visits [ 15 ]. Preventive–promotive home visiting services have been offered for decades with the goal of maintaining and promoting the health and independent functioning of older adults. In addition, these services aim to reduce admission to hospitals or nursing homes and the associated economic burden [ 16 , 17 ].
Home visits allow health professionals to evaluate possible problems in the living environment of homebound older adults, assess their physical and mental health status, provide older adults with professional support, and refer them to specialist care if needed [ 17 ]. By reducing the risk of functional deterioration, these strategies are primarily structured to enhance the health-related QoL (HRQoL) of older adults, increase the possibility of continued independent living, and delay mortality [ 18 ].
Home visits have been shown to positively affect patient care and provider attitudes as well as increased satisfaction among homebound older adults and providers [ 19 ]. A previous study demonstrated that preventive home visits may have positive effects on QoL of older adults [ 20 ]. However, the variability in the study designs, participants, and outcome measures has made comparisons difficult. Liimata et al. (2019) conducted a randomised controlled trial (RCT) measuring the effects of preventative multidisciplinary home visits on HRQoL of older adults living independently. The team, which consisted of a nurse, a physiotherapist, and a social worker, observed a significantly slower decline of HRQoL in the intervention group, but this effect diminished after the visits ended [ 20 ]. In a separate publication from the same study, preventive home visits resulted in an improved HRQoL without incurring additional healthcare costs [ 21 ]. An effective prevention method aids in supporting quality of life among older adults. In a review on preventive home visits for older adults, Mayo-Wilson et al. (2014) analysed 64 RCTs involving older adults without dementia from database inception until December 2012. The study yielded high-quality evidence for decreasing falls but low-quality evidence for quality of life [ 22 ]. Thus, although an RCT demonstrated promising results on home visits, a review of multiple RCTs failed to observe significant results. In addition, although multi-professional preventive home visit approaches with thorough evaluation and collaboration among healthcare professionals may be more beneficial than home visits by a single professional, few studies have focused on this multi-professional preventive home visit approach [ 20 , 23 , 24 ].
Multi-professional preventive home visit interventions involve coordination between several health care professionals towards shared goals. Effective communication among the team members is crucial when the members work within the boundaries of their expertise and subsequently discuss progress in group sessions [ 25 ]. Previous systematic reviews have provided a mixed picture of the benefits of multi-professional home visiting services for older adults. Stuck et al. [ 26 ] and Touringy et al. [ 14 ] suggested that the multi-professional approach with follow-up visits was effective in identifying the needs of the older adult population. However, Mayo-Wilson et al. [ 22 ] demonstrated the challenges of concluding that preventive home visits result in reliable benefits, primarily due to variability in the study designs, participants, and intervention strategies of the preventive home visits approach.
In Malaysia, home visiting services for the older adult population are delivered by a multidisciplinary team and are primarily provided by the Ministry of Health [ 27 ]. The home visiting services offered in Malaysia include home-based treatment, pharmacy counselling, rehabilitation, and palliative services, which aim to ensure continuity of care at home, reduce hospital readmission, and improve QoL [ 28 , 29 ]. According to the National Health and Morbidity Survey (NHMS) 2018, a national community survey for elderly health in Malaysia, 28.6% of older adults perceived themselves as having poor QoL, 14.1% reported having at least one fall in the 12 months prior to the survey, 8.5% were diagnosed with dementia, and 11.2% were at risk of experiencing depressive symptoms [ 30 ]. Poor QoL in Malaysian older adults was found to be associated with lower education, depression, food insecurity, reduced functional status, and a lack of social support [ 31 ]. Hence, we seek to examine preventive–promotive strategies that specifically prevent or reduce the risk of developing dementia, depression, and falls, with the ultimate aim of improving QoL among the older adult population.
To our knowledge, the most recent systematic review of primary studies examining the multi-professional preventive home visit approach for older adults included studies conducted up to December 2012 [ 22 ]. Because the older adult population is rapidly growing, the number of studies describing the home visit intervention is increasing, and the methodological and reporting quality of these studies is improving. Hence, a comprehensive systematic review which includes recent studies is needed to provide new evidence on the effectiveness of multi-professional preventive–promotive home visits in improving QoL among older adults. This review may serve as a guideline for the healthcare professionals, policymakers, researchers, and institutions in designing and delivering interventions for older adults in future. Aligning health systems with the needs of the older adult population may help to promote healthy ageing in Malaysia in the long term.
This study aims to systematically assess the effect of a multi-professional home visit approach on QoL among older adults.
The present protocol has been registered within the PROSPERO database (registration number CRD42021234531) and is being reported in accordance with the reporting guidance provided in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) statement [ 32 , 33 ] (see checklist in Additional file 1).
Eligibility criteria
Types of studies.
Randomised controlled trials (RCTs), cluster randomised controlled trials (cluster RCTs), and observational studies (such as cohort, case-control, and cross-sectional studies) will be included. Quasi-randomised controlled trials (quasi-RCTs), which are often associated with a high risk of bias, and cross-over studies will be excluded. Case reports, guidelines, protocols, and short communication will also be excluded.
We will only include studies examining the older adults without dementia aged 60 years and above who reside in their own homes and receive treatment at primary care outpatient departments. We will exclude studies that involve older adults living in retirement homes or nursing homes.
Types of interventions
We will include studies that aim specifically to assess the following interventions:
- Home visits which aim to prevent or reduce risks related to ageing
- Home visits which utilise at least two of the following multidimensional approaches: medical, functional, psychosocial, and environmental evaluation of problems and resources, resulting in specific recommendations for solving observed problems and preventing new ones.
Types of outcome measures
Primary outcomes.
We will measure QoL using validated scales such as the WHO QoL Questionnaires, WHOQoL-BREF [ 34 ] and WHOQoL-OLD [ 35 ], the 19-item Control, Autonomy, Self-Realisation and Pleasure (CASP-19) questionnaire [ 36 ], the Older People’s Quality of Life (OPQoL) questionnaire [ 37 ], and the 36-item Short Form Health Survey (SF-36) [ 38 , 39 ].
Secondary outcomes
We will also analyse the effects of home visit interventions on the incidence of falls, depression, dementia, and emergency department admissions.
Exclusion criteria
We will exclude studies that involve follow-up visits for recent hospital discharge and studies targeting people with one specific illness.
Information sources
A comprehensive systematic electronic search will be conducted using these databases: PubMed, Ovid MEDLINE (R), the Cochrane Library, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Web of Science, ClinicalTrials.gov , the metaRegister of Controlled Trials, the Turning Research into Practice (TRIP) database, Open Grey, High Wire, the National Institute for Health and Care Excellence (NICE), and the National Institutes of Health (NIH). The search will be limited to English language articles published from January 2010 onwards.
In addition, cross-referencing will be performed, whereby the reference lists of articles will be scanned for relevant studies. We will hand-search Malaysian quality initiative or health systems project reports in the libraries of the Institute for Medical Research (IMR), Institute for Health Management (IHM), Institute for Health System Research (IHSR), Institute for Public Health (IPH), and Ministry of Health, Malaysia.
Search strategy
The search strategy will be based on the key components of the research question: population, interventions, and outcomes. It will include a mix of medical subject headings (MeSH) terms and free-text terms in the title and abstract search fields of the databases. The keywords will be related to the participants (e.g., aged, senior, older, elder, and geriatric), home care (e.g., house calls, home visits, and home care), and the outcomes (e.g., quality of life and accidental falls). Examples of the search strategy are presented in Additional file 2.
Selection of studies
Two review authors will examine the titles and abstracts independently and will exclude all irrelevant studies. Two review authors will independently retrieve and screen the full text of potentially relevant articles and identify those that meet the eligibility criteria. These steps will be recorded in an Excel table along with the reasons for study exclusion. To avoid duplication, data will be identified from the main source. Any disagreements that arise will be resolved through discussions with a third author. A PRISMA flow chart showing details of studies included and excluded at each stage of the study selection process will be provided [ 33 ].
Data extraction
Two reviewers will independently retrieve and record data in a data extraction form. Any disagreements will be resolved through discussion with the third reviewer. The data extraction form will include the following variables:
- General information: title, first author, publication year, and country
- Methods: study design, study duration, sample size, and mean age of the sample
- Types of intervention: visitors’ professional group, number of visits, length of visits
- ○ Primary outcome: QoL (characteristics of the scales used to measure QoL)
- ○ Secondary outcomes: incidence of falls, depression, dementia, and emergency department admissions
Quality assessment
Two reviewers will evaluate the possible risk of bias for each study independently. Any disagreements will be discussed with the third reviewer. We will evaluate the RCT and cluster RCT articles for the methodological quality using the Cochrane risk of bias tool (RoB 2.0) [ 40 ]. We will categorise the risk of bias as low, high, or unclear in each of the following domains: allocation concealment, random sequence generation, blinding of outcome assessment, selective outcome reporting, incomplete outcome data, and other sources of bias.
The quality assessment tool for studies with diverse designs (QATSDD) [ 41 , 42 ] will be utilised to assess mixed-method studies. There are 14 QATSDD evaluative indicators for quantitative studies. Each indicator will be measured on a 4-point Likert scale as follows: 0 (not at all), 1 (very slightly), 2 (moderate), and 3 (complete). The maximum score of this tool is 42. The quality of a study is rated as ‘high’ if the score is over 75%, ‘good’ if it is between 50 and 75%, ‘moderate’ if it is between 25 and 50%, and ‘poor’ if it is below 25%.
Data synthesis and analysis
If the studies are sufficiently homogenous in terms of population, interventions, and outcomes, the results will be pooled, and a meta-analysis using a random-effects model will be conducted. Where possible, dichotomous data will be presented as relative risks (RRs) with 95% confidence intervals (CIs). Continuous data will be expressed as mean differences (MDs) or standardised mean differences (SMDs) (when the outcome is measured using several scales or instruments) with 95% CIs [ 43 ]. If the study characteristics are substantially different, the results will be analysed in the following subgroups, if data are available:
- Participant’s age: 60–79, ≥80
- Visitors’ professional group
We will interpret the heterogeneity and variability of the included studies in relation to population, interventions, outcomes, and methods. When meta-analysis is attempted, heterogeneity will be evaluated by forest plots to assess whether the CIs overlap. In addition, heterogeneity among the included studies will be measured using the chi-square ( χ 2 ) test and I 2 statistic. A small p value ( p < 0.1) for the χ 2 test and an I 2 of 50% or higher indicate moderate to substantial heterogeneity [ 44 ].
If meta-analysis is not possible, a narrative will be developed to summarise differences. We will present the data in a summary table outlining the content of the included primary studies (the number of participants, study population, description of interventions), as well as the results, conclusions, and quality ranking of studies.
Meta-bias(es)
We will assess publication bias using the Tandem method. If possible, the potential for reporting bias will be further explored using a funnel plot. A linear regression test will be performed to examine the degree of publication bias. Publication bias is significant if the p-value is less than 0.1.
Confidence in cumulative evidence
The quality of the evidence synthesised in this review will be assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology [ 45 ]. This methodology involves the evaluation of the evidence quality for each outcome across the domains of risk of bias, consistency, directness of evidence, precision of effect estimates, and publication bias, resulting in the following grades for each outcome: high, moderate, low, or very low [ 17 , 46 ].
This review may serve as evidence to support effective interdisciplinary home visits that can improve health-related QoL among older adults. This will potentially benefit policymakers and healthcare managers in planning for an efficient resource utilisation and evidence-based policy designs catered to older adults’ health. Healthcare professionals and implementers will be able to deliver health programmes and interventions suited to the needs of the older adult population. Researchers and other institutions will gain knowledge of multiple health interventions. In addition, recognising international practices will provide information to policymakers regarding strategies to improve quality of care in future.
This review has potential limitations. Our search strategy may miss sources of information available in languages other than the English language. In addition, we anticipate that the review will face challenges due to the heterogeneous nature of the study design, particularly in interventions and outcomes measures, which may limit the interpretability and comparability of results.
Protocol amendments
Any amendments to this protocol in the carrying out of this systematic review will be documented and reported in both the PROSPERO register and any subsequent publications.
Dissemination plans
The findings of this systematic review will be disseminated through publication in peer-reviewed journals and via relevant conferences. In addition, the results will also be shared with potential stakeholders, such as the Ministry of Women, Family and Community Development and the Family Health Development Division under the Ministry of Health Malaysia.
Acknowledgements
We would like to express our appreciation to the Director General of Health Malaysia for his permission to publish this systematic review protocol. We would also like to thank the Director of the Institute for Health Systems Research, National Institutes of Health Malaysia for her permission to conduct this review.
Abbreviations
Authors’ contributions.
Conceiving the protocol: YLT, NSAB, and ZA. Designing the protocol: YLT and NSAB. Coordinating the protocol: ZA. Designing search strategies: YLT, NSAB, and NAAMM. Writing the protocol: YLT, NSAB, RT, NHAR, and ZA. Providing general advice on the protocol: WKY. The authors read and approved the final manuscript.
The authors declare that they have received no specific funding for this work.
Availability of data and materials
Declarations.
This systematic review protocol was registered with the National Medical Research Register (NMRR-20-1810-56054), Ministry of Health Malaysia. Ethical approval was sought from the Health Medical Research Ethics Committee (MREC), Ministry of Health Malaysia, on 9 September 2020.
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Yea Lu Tay, Email: [email protected] .
Nurul Salwana Abu Bakar, Email: [email protected] .
Ruzimah Tumiran, Email: [email protected] .
Noor Hasidah Ab Rahman, Email: [email protected] .
Noor Areefa Ameera Mohd Ma’amor, Email: moc.liamg@areemafeeraroon .
Weng Keong Yau, Email: moc.liamg@kwuayrd .
Zalilah Abdullah, Email: [email protected] .

Join Us in Celebrating 50 Years of Dedication Towards Ending Isolation and Loneliness in the Lives of Seniors!
Friend to Friend America is celebrating its 50th year of service, dedicated to ending isolation and loneliness in the lives of seniors living in long term care communities. We couldn’t have reached this milestone without the incredible support and contributions from individuals who share our passion for creating meaningful connections and improving the lives of seniors.
Over the past five decades, Friend to Friend America has tirelessly worked towards fostering companionship, social engagement, and emotional well-being among seniors. We firmly believe that no one should feel alone or isolated, especially during their golden years. Our dedicated team, volunteers, and supporters have made a significant impact on countless lives, bringing joy, laughter, and friendship to seniors in need.
Our Mission
To end loneliness in the lives of seniors, one senior at a time, “Friend to Friend”. Friend to Friend America recruits and trains volunteers in the community to visit lonely and isolated seniors.
Friend to Friend America Can Help
Would you like a visitor? Do you know someone that could benefit from a visiting friend? Are your parents or grandparents living miles away? Are you unable to get there to visit as often as you would like? Would your relative enjoy the company of a friend? Fill out our request form today! Please note, at this time, our service area is limited to Washington State.
We are a 501 (c) (3) Non-Profit and nearly 100% volunteer staffed. Friend to Friend America depends entirely on individual donations and grants for its support. The nature of the program does not lend itself to charging for ‘services.’ Don’t have time to volunteer but still want to help? Please donate today!
Volunteer Today
Friend to Friend America recruits and matches volunteers to visit (one-to-one) with elderly and disabled persons who live in nursing, assisted living, retirement, and adult family homes to form friendships. The volunteer friends commit to visiting at least twice a month at their convenience for a minimum of one year. Anyone may volunteer; a background check and training are required. We are sorry, but we cannot assist with court-ordered community service. Do you have the heart to serve? Please get in touch with us at [email protected] for an application.

In-Home Dental Care for Homebound Geriatric Patients
Treating patients coast to coast, partner brands, become a house call dentist, we now have a mobile app.
Uber for Dentistry! Consult One Of Our Providers From Your Smartphone, Get Care Via Teledentistry, Or From Your Home Limited Availability*
Featured in:

Our Mobile Dentists Serve Patients Across the USA Many Locations Coming Soon!
Geriatric House Call Dentistry is committed to serving the most important generation of our time, and those who cannot receive dental care the traditional way. Dentists featured on our website are highly skilled in their field and operate their own practice independently in their respective locations. We are all highly trained independent practice owners providing dental treatment to our homebound elders. This is not a franchise. If you are a dentist who is interested in caring for an underserved aging population, please contact us for more information on the application process.
Manhattan & The Hamptons, NY
Dr. alisa kauffman, long island & queens ny, dr. rachel klein, chicago, il, dr. joy v. poskozim.
- Connecticut
Dr. Desiree Outlaw
Philadelphia, & surrounding counties, pa, dr. abby neville, brooklyn & staten island, ny, dr. raphael mosery, san francisco, ca, dr. weber & dr. bautista, suffolk county, ny, dr. craig lessinger, boca raton, fl, coming soon, sarasota & manatee co, fl, dr. antoine chiha, dallas fort worth, tx, dr. anshu bansal, phoenix arizona, now accepting patients.
- Seattle, Washington
Dr. Ajay Kashi
Milwaukee, wisconsin, dr. mihaela popa, nashville, tennessee, dr. uju nwizu, join our network, brands we believe in.
Vetted and advocated for by Dr. Kauffman, CEO of Geriatric House Call Dentistry. Click on the links below to learn more:

In Home Mobile Dental Services
Serving patients who may be homebound, bedbound, or may have a form of dementia. Our dentists are compassionate, empathetic, and highly skilled in their field. View our traveling dentistry services below, and contact your nearest provider to request a consultation or care.
Mobile Dentistry
Denture fabrication, denture repair, dental exams.
- Second Opinions
- Teeth Cleaning
Crowns (Caps) and Bridge Repair
- Cavity Treatment
Tooth Extractions
Emergency dental service.
- Teledentistry for Elderly Patients

Podcast: Knowledgeable Aging

The Suave & Sassy Seniors Show

Students of Smiles for Life

Souls Of NY

A Day in The Life of Dr. Kauffman

Dr. Kauffman Making Housecalls

Video Testimonial 1

Video Testimonial 2

Patient Comfort and Mobility

Recommended Products

Treating Geriatric Patients
What our patients have to say.
“ “ Dear Dr. Kauffman, Thank you so much for taking care of my 92 year old mother’s dental needs. Your professional and compassionate manner allow my mother to remain calm and cooperative while you are working on her. We are so lucky to live in New York where dentists like you exist. I certainly hope you can train others to do what you do, as there is an incredible need for the services that you provide to the geriatric and dementia population. You have such a great insight into this challenging, yet rewarding niche in the dental field that will only continue to increase in demand as our general population ages. Under your expert care my mother has all her own teeth and a beautiful smile! Finding you was such a blessing. Your understanding of the challenges and needs of our seniors as it pertains to good oral and overall health has helped us immensely in our daily dental care routine. Thank you for all that you do for your patients and their families. ” Evelyn Versace
“ “ We were lucky to find Alisa but it was difficult. My wife Susan, Sweet Susan, has Alzheimer’s Dementia. Finally, about 3 years ago, her family Dentist of many years told me he could no longer treat her because she could not follow his directions and we needed a Dentist who could sedate her! ” My Wife Susan
“ “ Dear Dr. Kauffman, We thank you for the amazing job you did restoring our sister’s smile! ” The Osea Family
“ “ Dr. Kauffman is responsive, compassionate and provides efficient care. Her follow up care and concern for her patient was exemplary! She saved the day and we were able to celebrate my mother’s 100th birthday. Thank you, ” BETHANY
“ “ Thank you a million Dr. Kauffman. This is my best Christmas in many years. You are my angel. -Carl A. ” CARL A
“ “ I cannot believe how beautiful my grandmother’s dentures look and fit. We only wish we found you sooner s she would have had more years to smile and eat effectively! God Bless You for providing this unique service. ” PAUL L
“ Dear Dr. Kauffman, Alan is doing well. I think he must have been in pain with the loose tooth because he has been very quiet and seems to feel good since you pulled the tooth. He used to moan a lot, and would eat very slowly. I usually had to feed him after he took a few bites. He has not moaned this afternoon. He had a nap in his recliner, and he ate a good lunch and dinner easily and he fed himself. I am so happy that you treated him.. II think it made a big difference in him. Lucinda agrees with me. Thank you. Also, no bleeding. I gave him his coumadin at seven. All is well, for sure Thank you very much. ” ALAN IS DOING WELL
“ “ Dear Doctor Kauffman, I wanted to let you know that our mom passed away this morning. As you know she’d been a long slow decline and today it caught up with her. She passed away with all her teeth but one, thanks to your good care and her good genes! You were a godsend during these last few years when we couldn’t get her to the dentist. Thank you for your care and kindness. Sincerely, Alison and Babette Lazarus ” ALISON AND BABETTE LAZARUS
“ I have general anxiety disorder and am very scared of the dentist .. I don’t travel from home and I contacted Dr. Alisa Kauffman for advice and she went above and beyond to help me. I truly recommend her to all. Thank you -S.K. ” S.K
“ Dear Dr. Kauffman, My entire family thanks you for the wonderful treatment you provided for my husband with Alzheimer’s Disease. We were frustrated that he would not cooperate for his dentist of 20 years, but miraculously you were able to make him new well fitted dentures that he doesn’t want to remove. And in this freezing cold weather you were able to do the entire process in our apartment. Whoever doesn’t believe in miracles needs to meet you. We thank you for your patience and kindness and wish you all the best with your newest endeavors. Kindest regards, -Dolores D. and family ” DOLORES D. AND FAMILY
“ “ Thank you so much for your patience and for giving me my smile back! ” Thank You!
“ “ Thank you so much for having the compassion and energy to do this type of work. I’m watching one of your videos as I write this! How fantastic and joyful you are. I wish I’d been there to see you in person. Please know I thank you from the bottom of my heart. -Wendy L. ” WENDY L
“ Hi Dr. Alisa I thought you would want to know that my mother passed away on Saturday afternoon. Thank you so much for the wonderful care you gave her. The mouth guard worked really well. So well, in fact, that for the last several weeks, Margaret said she had stopped grinding her teeth. We very much appreciated your concern and your kind and gentle treatment. Wishing you and your family the very best for this coming New Year. Debbie ” DEBBIE
“ Thanks so much for treating my mother. When I woke up in the middle of the night and saw you on PBS, it was a dream come true. I’ve been concerned about my mother getting dental care, because I know how important that was to her and my dad. So thanks for fulfilling that need. -Leslie Hoff ” LESLIE HOFF
“ Thanks so much Dr.Kauffman for the care you provided for my 95 year old mom. In a time whe medical and dental care is a business,fiding a caring and dedicated professional whose first prioity is the health of her patient is truly and answer to our prayers. Thanks so much from the bottom of my heart. From S. Hall. ” S. HALL
“ Alisa I read with great appreciation the article about your mobile dentistry in a magazine Igor shared with me. Even though it has been a long time since Willene and I were your patients, I remember the deft, precise work you performed. The article was so descriptive of your person that I felt I was once again in your chair. I was surprised when you left the practice. Fortunately, Igor’s architecture has precluded the need for your new services. But as a professor of innovation and entrepreneurship, I truly applaud your creative choice to fulfill an unmet need in a way that few are capable of doing. I wish more professionals would emulate your passionate, creative service. Frank PS Igor also told me about all your good work at Penn, which is my favorite Ivy. ” FRANK H.
“ “Dr. Kauffman is a real angel. What a beautiful gift of needed service for her patients.” “So many services, such as dentistry and optometry are lacking in nursing homes and for shut-ins. My father’s glasses were mangled when the nursing home aides allowed them to drop to the floor where they were crushed when the aides moved dad’s bed. He couldn’t see without them. Somehow we managed to get the frames bent back into shape, but there was no way to get him fitted with new glasses. The world needs more practitioners like Dr. Kauffman.” “This is a brilliant service. Dental care is overlooked for the elderly yet vital for healthy aging. As we encourage more people to age in place, serving this home-bound population will become socially critical and lucrative for businesses.” “What a really wonderful breath, of fresh air to see such a story. Dr. Koffman thank you for your compassion and dedication in treating those in need. Being this is such a unique story and one that beams integrity, I have added your story to a page that honors professionals such as yourself. http://www.welcometodds.com/medical-hall-of-fame Thank you again for your exemplary service and for teaching others to follow suit.” ” WASHINGTON POST TESTIMONIALS THESE TESTIMONIALS WERE TAKEN FROM COMMENTS ON THE WASHINGTON POST.
“ “ My Dad is 100 years old. He developed dementia a few years ago. Recently his dentures broke in half, and a tooth went missing. Not having dentures made mealtimes challenging. His food needed to be mashed to make it easier for him to eat. Speaking was a little difficult for him too. Not to mention, at 100 years old, he couldn’t understand why we took his dentures away; He kept asking for them. We tried a couple of neighborhood dentists but they rejected him: either they didn’t accept his insurance or simply weren’t equipped to work with geriatric patients. With that, my sister decided to surf the net in search of a geriatric dentist. Lo’ and behold, she came across Dr. Alisa Kauffman, DMD. I immediately called Dr. Kauffman, and without hesitation, she assured me that she could replace the missing tooth, repair the dentures, and overnight them back to my Dad via Fed Ex. Wednesday afternoon my brother-n-law dropped off the dentures, and by Friday morning my Dad was back to his ol’ self again; smiling, eating and talking. He was on top of the world. We are all grateful for Dr. Alisa Kauffman’s professionalism, and punctuality. We are especially thankful for the compassion, care and commitment she has for the elderly. Thank you Dr. Alisa Kauffman, DMD for my Dad’s bright smile. Seeing Pop happy makes us happy. You are phenomenal! Molly Barreto & Family ” MOLLY B & FAMILY
“ “ Dear Dr. Kauffman, I can’t thank you enough for helping me in a time of crisis!!! I couldn’t eat or smile until you were able to fix my teeth ! And thank you even more for doing it so quickly. God bless you and I hope you inspire more of your students at University of Pennsylvania to become housecall dentists. Sincerely, Margaret Lipton ” MARGARET LIPTON
“ “ Dear Dr. Kauffman, I want to thank you from the bottom of my heart for making me new teeth. I was so depressed when the hospital lost my dentures, but you gave me hope and my dignity back by replacing them with even better fitting dentures than before. God bless you and I feel blessed that I met you. Best of luck and your future patients should know that they are in such capable hands. Sincerely, Patrick Rogan NYC ” PATRICK ROGAN
“ I am writing to express my sincere thanks and appreciation for your patience and excellent work in making a replacement denture for my mother, who is a resident at Schervier Nursing Care Center in the Bronx. As you know, the use and safeguarding of dentures for persons with dementia presents significant challenges for the patient, families and nursing homes. In my mother’s case, her partial denture was lost after about a year in the nursing home. Soon after, she began grinding her teeth involuntarily causing damage to her upper and lower incisors. After a referral was made to you by the nursing home, you expeditiously worked with me, the nursing home staff and my mother to create a replacement denture. In addition, after the replacement denture was completed, you patiently dedicated time to instructing me as well as the nursing home staff on the proper methods for removing, cleaning, re-inserting and, as importantly, safeguarding the denture. My mother is no longer grinding her teeth! I am so very grateful to you. Bravo! Carlos M. Diaz ” CARLOS M. DIAZ
“ “ Dear Dr. Kauffman, The video you showed us in 3rd year class at UPenn was hilarious. I remember the very groovy background music – that lecture was a blast! The geriatric rotations made me think about what a mobile practice “setting” can be and got me thinking of doing something similar in the future. As a graduate from the class of 2015, I am currently working with a large Indian Health Service hospital in Fairbanks, Alaska. I have the privilege of being part of a very unique team of dental professionals servicing a patient base of ~34,000 patients spanning more than two dozen villages spanning an area the equivalent of Texas, and reaching as far north into the Arctic. I provide routine and emergency dental care which includes general, endodontics, prosthodontics, periodontics, pediatric, and oral surgery dental care. Prior to graduation I also completed an externship in Barrow, Alaska, which was my starting point for an interesting career. On a daily basis I interact with Community Health Aide Practitioners and Dental Health Aide Therapists (a controversial public health initiative which has immense success in Alaska – feel free to reach out to me if you are interested in learning more). I also coordinate medical evacuations for dental patients living in the remote villages. Furthermore, an important aspect of my job is to travel to remote villages via small bush planes (through harsh Arctic winter weather! And as part of this job I even signed a “death by travel waiver.” ) in order to deliver mobile dental services to village patients, with a focus on pediatric and geriatric segments – one of the most enjoyable aspects of the job is to listen to village elders describe stories of their pre-electricity lives while I perform their denture treatment! It is this aspect of the job that motivates me to become a geriatrician: an often overlooked dental need working with a patient population with both immense amounts of medical/dental needs and wisdom to share with us. As dental needs become much more accessible to a geriatric patient base, the options and affordability for home- and mobile-based dental care is likewise poised to expand, both in private and public sectors ” STEVEN LIN
“ “ Dear Doctor Kauffman, I wanted to let you know that our mom passed away this morning. As you know she’d been a long slow decline and today it caught up with her. She passed away with all her teeth but one, thanks to your good care and her good genes! You were a godsend during these last few years when we couldn’t get her to the dentist. Thank you for your care and kindness. Sincerely, Alison and Babette Lazarus ” VICTOR L
“ Congratulations on the fabulous article regarding the life-giving work and comic adventures of Dr. Alisa Kauffman. Such a tremendous understanding of the needs of our elderly, and the ability she obviously has to deliver that care, is quite admirable. I am proud to note that there are many institutions scattered throughout North America, Israel, and beyond, that cater to the elderly and particularly to Holocaust survivors – but none perhaps with the flair of Dr. Kauffman. Thank you for bringing this all to our attention. May Dr. Kauffman, and those like her, continue their sensitive and so vital work in good health, good strength, and good spirits. ” Gary Charlestein Taken from the Pennsylvania Gazette, July/August 2017 Edition
“ “ Dr. Alisa Kauffman is not just an outstanding dentist, but a devoted, caring, and dedicated professional. My 103 year old aunt, Doris (photo is from her 102nd birthday party), required urgent dental care at home, including multiple root extractions in order to remedy an infection and enable her to chew food comfortably and safely. Although Doris was a new patient, Dr. Kauffman rearranged her vacation schedule to ensure that Doris was treated in a timely way. Dr. Kauffman spent time in advance of the visit to make certain she understood my aunt’s health, mental, and psychological condition. She treated Doris in an exceedingly caring manner, with dignity and respect often lacking in today’s fast-paced medical encounters. She has a reassuring and calming presence which is vital for all patients, and most especially for the elderly. She made sure that Doris understood the treatment plan and encouraged her to ask questions. Doris was feeling 100% better the following day. We are very grateful to Dr. Kauffman! ” DORIS
“ Alisa Kauffman travels the urban frontier alone. She brings attention to a need for the coordination of comprehensive dental/medical services for the elderly. As the population continues to age, these critical services need to be readily available for non-ambulatory patients. The challenge is for Penn – the national leader in geriatric care for over 150 years – to better utilize its resources in dentistry, medicine, and research to help the elderly and often home-bound community. ” Marcia Witlin-Basickes Taken from the Pennsylvania Gazette, July/August 2017 Edition
“ “ I would like to give my highest commendation to Dr. Alisa Kauffman. She came highly recommended to me by my own dentist when I was in need of a dentist who would treat my bed/wheel chair bound husband at home. My husband had suffered traumatic brain injury and profound physical disability as the result of an accident making it impossible to transport him to a dental office. Dr. Kauffmann was happy to visit my husband at home. Her manner is thorough, knowledgeable and exceedingly professional. She has assured me that should he require extensive dental work, she will coordinate everything for us, which has allayed any anxiety I may have had. She comes to our home on a regular basis which she schedules, to maintain my husband’s oral hygiene. As a psychologist, I am extremely impressed not only by her professional expertise, but with her extraordinary ability to engage my traumatic brain injured husband. He is always delighted to see her, looks forward to her visits and cooperates fully while she is working on his mouth despite any discomfort he may experience in the process. ” ELIZABETH T. KLONER, PH.D. KNOWLEDGEABLE & PROFESSIONAL.
“ “ I want to thank Dr. Kauffman for making me look pretty with the beautiful teeth, so I can smile! ” URSULINA PADUVANI WANT TO THANK DR. KAUFFMAN
“ “ Hello, my name is Richard. I am a client of Dr. Kauffman, who is my dentist. When she did my dental, she set up everything and made it right here in the house! That service is a great thing because I cannot get out. ” RICHARD WEINKAUF SHE DID MY DENTAL, SHE SET UP EVERYTHING
“ “ Dr. Kauffman, I am in my 90’s and you made me look younger. Thank you so much! ” JR
“ “ I just want to thank you for all the wonderful dentistry you have done for me over the years, You made me feel comfortable by taking so much time explain the procedure you were doing, You are a fantastic qualified geriatric dentist, but equally important an amazing woman. I wish you a long and happy career. ” DORIS HERING YOU MADE ME FEEL COMFORTABLE
“ “ Dr. Kauffman: very professional, you know exactly what you’re doing and her nickname for you is the painless dentist – what more can you ask for? Thanks again, Mollie ” MOLLIE
“ “ Dear Dr. Kauffman, Thank you for coming to my apartment to get my smile back in order. I thought I would never see a dentist ever again since I have such limited mobility which makes it difficult to get to my dentist. But a visiting dentist who can do all the work in my apartment solved all my worries!! I also really appreciate that you called my old dentist to coordinate treatment as he originally planned it I really looked forward to my dental visits, and I could always count on you to come over as promised. Thank you for listening to all my stories and I am proud to share my BEFORE and AFTER photos with you. Thank you again for all your excellent work! William Smith. ” WILLIAM SMITH
“ Dr. Kauffman is such a unique person. Not only is she the best dentist, she brings to the home-visit a feeling of happiness, caring, and makes everyone confident that everything will be ok. As a geriatric social worker I have made many home-visits with Dr. Kauffman. My clients (some are bed bound) are sometimes nervous thinking about how a visit could be done by a dentist in the home. From the minute she walks into the bedroom and gives the biggest hello, my clients smile back and I can see they become relaxed and happy and confident to be treated by such a warm person. I wish all dentists were like Dr Kauffman. Sasha Greene ” SASHA GREENE " I WISH ALL DENTISTS WERE LIKE DR KAUFFMAN."
“ “ I have worked with Dr. Kauffman for about 20 years. My name is Harriet Duncan. I am a a nurse at Kingsbridge Heights Nursing Care Center. Dr. Kauffman is a very good dentist. She is very generous and patient. Satisfactory! No complaint! She is very good at working with the staff, with the patients, with everybody. She does a very good job. She is a good dentist! ” HARRIET DUNCAN SATISFACTORY! NO COMPLAINT!
“ “ Thanks for being pro-active Dr. Kauffman. And thanks as well for all to help us deal with her dental/grinding issues for the final years of her life was a great help and comfort to our family. So all of us send you our gratitude, on behalf of Seph, and the entire Melrod family! ” GEORGE MELROD THANKS FOR BEING PRO-ACTIVE
“ “ Thanks for publishing the fascinating piece on Dr. Alisa Kauffman [“House Dentist,” May 2017]. It’s alway refreshing to find there are people out there whose work – and attitude toward life – can put a smile on our faces. I hope the writers of the endless letters – pro or con – about our fellow alumnus, Donald Trump, read the article. A good many of them could stand to put a smile on their faces. Louis R Sernoff C’62 L’65 Delrey Beach, FL Taken from the Pennsylvania Gazette, July/August 2017 Edition ” Louis R Sernoff BE LIKE ALISA
“ I enjoyed reading ‘House Dentist’. I appreciate that you [Penn Gazette] highlighted the good work that Penn Alum’s do in their professions, with an eye towards service and underserved communities. I hope you write more articles like that in the future and thank you to Alisa Kauffman and Steven Lin [who was profiled in the sidebar article, “The Protégé”] ” Michael Chen Taken from the Pennsylvania Gazette, July/August 2017 Edition
“ I just wanted to say on behalf of Molly Barreto and all of our family we truly appreciate you taking care of Emilio Barreto. He is my grandfather and as is suffering Alzheimer’s and as a result life is difficult and complicated at times. With your help and encouragement he has one less daily struggle and for that I am completely grateful. -Amanda ” AMANDA One of Emilio Barreto’s grandchildren
“ Dearest Alisa, Thank you for your very sweet email. You made yesterday such a pleasure. I wish everyone I had to deal with in my life could be just like you. You are beyond sweet and lovely. I wish I could have known you prior to this happening to me. Thank you again. Lovingly, Leslie ” LESLIE
“ “ Dear Dr. Kauffman, You made the impossible treatment happen and I have the perfect result. I am eternally grateful for everything you did for me. You are truly a master dentist and there should be more people like you to help others like me! Best, Elizabeth Philbin ” ELIZABETH P
“ “ Thank you Dr. Kauffman for making me feel great again. Love, Sarah ” SARAH
Geriatric Products We Believe In!
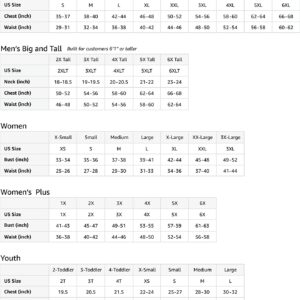
Womens Caregiving I'm A Caregiver What's Your Superpower Nursing T-Shirt
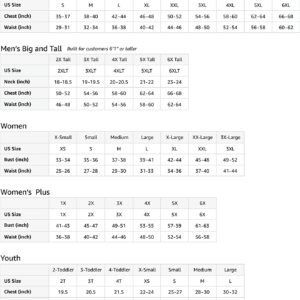
Baby Boomer Funny Humorous Slightly Older Senior Citizen T-Shirt

Dr. B Dental Solutions Ultrasonic Cleaner, High Frequency Wave Cleaning Machine for Dentures, Nightguards, Retainers, Aligners, and Sleep Apnea Devices
Dr. B Dental Solutions Ergonomic Denture and Mouth Toothbrush, Extra Soft Bristles Removes Adhesives, Food, Stains and Odors, Single White Pack

Dr. B Dental Solutions Cleanadent Dental Wipes, Denture Cleaner Removes Adhesives, Food, Stains, and Odor 30 Count Pack

Dr. B Dental Solutions Liquid Crystal Soak Cleanser

MyFitStrip Dental Pro, Prebiotic Nitric Oxide Chewing Gum with Vitamin C, Zinc, and Xyitol – Promotes a Healthy Oral Microbiome and Alkaline pH – Sugar Free – 8 Cool Mints Tablets

Epic Xylitol Chewing Gum – Sugar Free & Aspartame Free Chewing Gum Sweetened w/ Xylitol for Dry Mouth & Gum Health (Cinnamon, 1000-Piece Bag, 1 Bag)
© 2024 Geriatric House Call Dentistry. Geriatric House Call Dentistry is committed to serving the most important generation of our time, and those who cannot receive dental care the traditional way. Dentists featured on our website are highly skilled in their field and operate their own practice independently in their respective locations. We are all highly trained independent practice owners providing dental treatment to our homebound elders. This is not a franchise. Dr. Kauffman recommends and distributes denture products by Dr. B Dental Solutions. Website and web marketing by Syndicate Marketing Agency
- House Call Dentures
- Dentistry for Assisted Living Centers
- Denture Fabrication and Repair
- Tighten and Repair Loose Dentures
- Comprehensive Dental Exams
- Repair & Re-cement Crowns, Caps, and Bridges
- Extraction for Elderly Patients
- Emergency Dental Service for Elderly
- Rated a Top 25 Dentist
- Dr. Klein – Queens & Long Island, New York
- Dr. Joy V Poskozim – Chicago, Illinois
- Dr. Mosery – Brooklyn & Staten Island, New York
- Dr. Outlaw, Connecticut
- Dr. Neville – Philadelphia & Bucks County, Pennsylvania
- Dr. Bautista & Dr. Weber – San Francisco, California
- Dr. Anshu Bansal – Dallas, Fort Worth Texas
- Dr. Craig Leshinger – Suffolk County, New York
- Dr. Antoine Chiha – Sarasota, Florida
- Dr. Candace Gershkovich & Dr. Sohrab Danaei – Phoenix, Arizona
- Dr. Ajay Kashi – Seattle, Washington
- Dr. Mihaela Popa – Milwaukee, Wisconsin
- Dr. Nwizu – Nashville, Tennessee
- Join our team and become a house call dentist
- Leadership Team
- Dementia Toothbrush
- Manhattan, New York
- The Hamptons, New York
- Queens, New York
- Long Island, New York
- Brooklyn, New York
- Staten Island, New York
- Suffolk County, New York
- Chicago, Illinois
- San Francisco, California
- Philadelphia, Pennsylvania
- Bucks County, Pennsylvania
- Los Angeles, California
- Boca Raton, Florida
- Dallas Fort Worth, Texas
- Sarasota and Manatee County Florida
- Naples, Florida
- San Antonio, Texas
- Phoenix, Arizona
- Nashville, TN
- Request a new location
- Request an Interview with Dr. Alisa Kauffman
- New York Times
- Women in Dentistry
- Washington Post
- Dental Products Report
- Dental Economics
- Podcast: Who’s Here in the Hamptons
- CaringKind, The Heart of Alzheimer’s Caregiving
- Smiles For Life
- Suave & Sassy Senior Show
- CaringKind NY
- Straight Talk: Vicki Schneps and Geraldo Rivera
- ABC: Covid-19
- This Is Me, Francoise
- Souls of NY
- Featured News Clip 1
- Featured News Clip 2
- Chicago Tribune
- Penn Gazette
- Penn Dental Medicine
- WFUV 90.7 Radio
- Dentistry to Seniors
- Coterie Hudson Yards
- Elevate Oral Care
- Geriatric Products
Home health services
Medicare Part A (Hospital Insurance) and/or Medicare Part B (Medical Insurance) cover eligible home health services as long as you need part-time or intermittent skilled services and as long as you’re “homebound,” which means:
- You have trouble leaving your home without help (like using a cane, wheelchair, walker, or crutches; special transportation; or help from another person) because of an illness or injury.
- Leaving your home isn’t recommended because of your condition.
- You’re normally unable to leave your home because it’s a major effort.
Covered home health services include:
- Medically necessary part-time or intermittent skilled nursing care
- Physical therapy
- Occupational therapy
- Speech-language pathology services
- Medical social services
- Part-time or intermittent home health aide care ( only if you’re also getting skilled nursing care at the same time)
- Injectable osteoporosis drugs for women
- Durable medical equipment
- Medical supplies for use at home
A doctor or other health care provider (like a nurse practitioner) must have a face-to-face visit with you before certifying that you need home health services. A doctor or other health care provider must order your care, and a Medicare-certified home health agency must provide it.
In most cases, "part-time or intermittent" means you may be able to get skilled nursing care and home health aide services up to 8 hours a day, with a maximum of 28 hours per week. You may be able to get more frequent care for a short time if your doctor or other health care provider determines it's necessary.
Medicare doesn't pay for:
- 24-hour-a-day care at your home
- Meals delivered to your home
- Homemaker services (like shopping and cleaning) that aren’t related to your care plan
- Custodial or personal care that helps you with daily living activities (like bathing, dressing, or using the bathroom), when this is the only care you need
You're not eligible for the home health benefit if you need more than part-time or "intermittent" skilled nursing care . You may leave home for medical treatment or short, infrequent absences for non-medical reasons, like attending religious services. You can still get home health care if you attend adult day care.
Your costs in Original Medicare
- $0 for covered home health care services.
- After you meet the Part B deductible, 20% of the Medicare-approved amount for Medicare-covered medical equipment.
Before you start getting your home health care, the home health agency should tell you how much Medicare will pay. The agency should also tell you if any items or services they give you aren't covered by Medicare, and how much you'll have to pay for them. This should be explained by both talking with you and in writing. The home health agency should give you a notice called the Advance Beneficiary Notice" (ABN) before giving you services and supplies that Medicare doesn't cover.
If you get services from a home health agency in Florida, Illinois, Massachusetts, Michigan, or Texas, you may be affected by a Medicare demonstration program. Under this demonstration, your home health agency, or you, may submit a request for pre-claim review of coverage for home health services to Medicare. This helps you and the home health agency know earlier in the process if Medicare is likely to cover the services. Medicare will review the information and cover the services if the services are medically necessary and meet Medicare requirements.
Your Medicare home health services benefits aren't changing and your access to home health services shouldn’t be delayed by the pre-claim review process. For more information, call us at 1-800-MEDICARE.
Things to know
During the COVID-19 pandemic, nurse practitioners, clinical nurse specialists, and physician assistants can provide home health services, without the certification of a physician.
Related resources
- Medicare & Home Health Care
- Find home health services
- More about home health care
- Your rights as a home health patient
- Complaints about your home health agency
- How will I know if the agency is reducing or stopping my services?
- Medicare & You: home health care (video)
Is my test, item, or service covered?
Home Visits
Home visits have been one of the social worker’s most effective tools from the very beginning. Examining the home provides information you can’t get in any other way.
Decades ago, social workers called themselves “friendly visitors” when they left the office to visit a client’s house. Their job was to get to know the family, to understand how its members interacted with one another, and to help the family overcome any problems it might be having.
Why Do We Need To Make Home Visits?
“An Adult Protective Services (APS) investigation is initiated by a visit to the vulnerable adult who is the alleged victim at the adult’s home or other place of residence.” ( 340:5-5-2. Policy )
If you don’t visit the client’s home, you may never discover problems that have gone unvoiced. There are many reasons someone might fail to tell you about a problem.
- Embarrassment
- Failure to See the Problem
When you make the home visit, you’re there to accomplish a specific goal that works toward the DHS Mission Statement of strengthening families and helping them become self-sufficient.
One of the many differences between DHS eligibility programs and APS is that it is not always the case that the client has requested our assistance. Social service needs easily arise, and since the client has not been in to report them, the home visit is one way those needs can be identified.
Getting Ready for the Home Visit
In general, it’s rarely a good idea to just jump in your car and head out for the field. Your time is limited, and you are obligated to make the best use of it as you can, both for your own benefit and that of those families you serve. While it may appear you’ve got a simple task ahead of you, and it’s not necessary to do a lot of preparation, taking a few moments to sort things out and examine your reasons for making the home visit will eliminate repeated visits as well as wasted time.
The following checklist may assist you:
- As part of the APS procedures and the investigative process, review and staff the referral with your supervisor.
- Have a plan.
- Gather your forms.
- List the client’s name, address and phone number on your ADM-57 for the day.
- Purses and other valuables should be placed in your trunk before you leave for the field.
- If you’re making multiple home visits, plan them so to economize traveling.
The home visit is one of your best opportunities to get to know the client you’re serving, and adequate preparation in the beginning will increase your likelihood of accomplishing that task.
Making the Home Visit
There are several things you need to keep in mind as you make the journey to the client’s home.
Here’s a quick checklist:
- Write your odometer reading on the ADM-57.
- Be professional.
- Don’t rush things.
- What if they’re not home?
- When you’re in the home, do not go exploring without the client’s permission.
- Before leaving, review what has been learned and what needs to be done next.
- When you leave the client’s home, go somewhere else to record your notes from the visit.
Use the time you are in the client’s home effectively.
Your objective is to assist the family. If you observe something that requires explanation, ask the questions necessary to resolve the issue.
Once again, the DHS Mission Statement says we’re here to help families become safer, healthier, more independent and more productive. Keep that mission in mind when you’re in the client’s home.
Any situation endangering the safety or health of the family may be critical enough to require immediate attention on your part.
Who Is At Risk?
When we first started this section on home visits, we noted the home visit’s importance in the process of getting to know a client’s needs.
While it is true many of the clients you’ll serve have unspoken needs, you need to be able to discern what it is that is placing the client at risk. Sometimes it is a lifestyle choice or another person’s influence or lack or care that is placing the client at risk and then there is the capacity of the client which is always a factor.
You will have to make judgment calls based on your own experiences, and you’ll discover you may have different concepts of what constitutes an acceptable or unacceptable situation when you discuss situations with your colleagues.
Though some of the situations you’ll encounter are going to be easily labeled as “at risk” or “not at risk,” you’ll find others fall into a gray area in which making a certain decision of risk factors will be like navigating through a thick fog.
You are in the business of providing protective and preventive services. In other words, you should know a client’s situation well enough to identify problem areas and assist in providing solutions to them whether they be minor or critical. Some client situations will require less intervention on your part than others. Some of the clients on your caseload will require no intervention at all. Once again, this points out the importance of your getting to know the client situation as well as possible. Assessing the client’s strengths and weaknesses requires information, and much of that information will only be available to you after you make a home visit.
Elderly and/or Disabled Individuals At Risk
As mentioned earlier, it’s a good idea to include a little extra time in your home visit for those who may be isolated from others. The elderly and/or disabled often find themselves unable to travel easily, and they may become dependent upon people coming to see them for social interaction. The time you spend with them may accomplish more good than you realize. Don’t treat it frivolously, and don’t squirm in your seat.
Many elderly and/or disabled individuals would benefit greatly from community resources designed specifically to meet their needs, but they may be unaware of them or unwilling to participate. Consider making appropriate referrals and providing encouragement to those who might be reluctant to take part in groups or activities that could help them become more active.
One third of your caseload will likely include elderly, disabled, and other vulnerable adults who are at risk and alleged to have abuse, neglect, and/or exploitation. Approximately two thirds of your clients will be suffering from self-neglect. If you do not make home visits, you may not recognize the client’s need for help. And policy does require “An Adult Protective Services (APS) investigation is initiated by a visit to the vulnerable adult who is the alleged victim at the adult’s home or other place of residence.” (340:5-5-2. Initiating investigations)
The Toll-Free Hotline number for Child Abuse/Neglect and Adult Abuse/Neglect is
1-800-522-3511.
- Core Values
- Our Dentists
- Caregivers & Families
- How It Works (Patients)
- New Patient Registration
- Medicare Advantage Programs
- PACE Programs
- Senior Communities & Group Facilities
- Texas Skilled Nursing Facilities
- HCS & Special Needs Facilities
- How It Works (Partners)
- In-Person Services
- Teledentistry
- Forms & Documents
- News & Blog
- Tooth Chart

Providing Portable At-Home Dental Services
Enable Dental provides at-home dental services for unique populations in the comfort of the patient’s home, senior home, assisted living facility or community center.
Enable Dental is easily accessible for homebound individuals. They respond quickly to concerns and are genuinely open to feedback. Enable Dental ensures vulnerable populations have access to much needed dental care.
It was nice meeting you and Dr Jenna, Miguel and Anet today, an amazing group of people! Everyone did their utmost to make my mother feel comfortable, she knew she was in good hands! Thank you for going out of your way to ensure that everything went smoothly and with a smile! Your positive energy and enthusiasm for what you all do, was evident today, as well as in the past, when I spoke with you on the phone. Considering the time you are on the road, dealing with multiple family members, and facility staff, it’s obvious that you enjoy your job and are very good at it! We are grateful for having you work so hard to get Mom back on track! Looking forward to seeing you all on the next visit.
The staff is very friendly, extremely knowledgeable, and have amazing patience. They are able to work with anyone and manage to keep not only a smile on their faces, but on the faces of their patients as well. I highly recommend this dentistry company.
Your crew are all professional, informative, and thorough. They provide an invaluable service that’s greatly needed by a segment of people who have little or no other options. Plus, they’re friendly and kind and so very considerate.

At Enable Dental, We Bring The full Scope Of Dental Care Directly To Our Patients.
We focus on providing top-tier clinical dental services in the comfort of our patient’s home or on-site community, significantly reducing the need for hospital visits and lowering the risk of infections.
- The removal for an escort and the associated risks.
We specialize in caring for seniors, individuals with memory issues and special needs, ensuring our services reduce stress for residents, their families, and caregivers by maintaining their routine in a familiar environment.
- Our services are adaptable and can be delivered in communal areas within communities, directly in residents’ apartments, or bedside for those requiring more intensive care.
- Enable Dental’s clinicians are equipped to provide a range of services, including exams, X-rays, cleanings, fillings, extractions, crowns, dentures, and more.
- Each patient’s dental and health history is thoroughly assessed to create a personalized care plan.
- We tailor each plan to meet the unique needs and preferences of each patient, ensuring the most effective and comfortable treatment and approach.
- We bring high-quality dental care to your doorstep, whether it’s at your home or an on-site community setting.
- With us, there is no compromise on quality or convenience; we bring the best of dental care to where you are most comfortable.
We Bring The Dentist To The Patient!
Our portable systems make it possible to thoroughly diagnose and perform dental treatment wherever the patient resides.
We create custom dental solutions suitable for your organization and budget.
Our patients are seen on a regular, recurring schedule. We manage and handle all the scheduling, care coordination, and billing.
The health and safety of our patients, team, and community is our utmost priority. Our clinical staff is fully vaccinated to COVID-19.
Catch The Enable Dental Team In Action

Expanding access to dental care for all
Using our mobile dental solutions model, Enable Dental provides all the dental services you would expect at a traditional office while allowing us to deliver high quality care to our patients at home.
We hope that our partnership can facilitate access to dentistry and ensure that oral health care can be made accessible to all under-served populations.
Our handheld digital x-ray units, custom dental chairs, and wheeled dental units make it possible to thoroughly diagnose and perform dental treatment in different living environments.
Our unique approach facilitates access to dentistry for all, and ensures that oral health care can be made accessible to unique and under-served populations.

At-home dentistry across the country
With over 20 locations across the country and 10 more opening soon, Enable Dental is ready to serve you and your community.
- 6500 Dublin Blvd ste 210
- 2414 S Fairview St ste 107a
- 1401 El Camino Ave
- 2414 S Fairview St
- Colorado Springs
- 1250 S Parker Rd
- 743 Horizon Ct suite 106
- 4500 Hiatus Rd
- 4500 Hiatus Rd suite 202
- 8367 Nieman Rd
- 250 N Rock Rd
- 8475 Sparta Line Rd
- 9500 Brooktree Rd
- 5555 N Lamar Blvd
- 12200 Ford Rd
- 15995 N Barkers Landing Rd
- 3700 Fredericksburg Rd
- 3813 22nd St ste 4c
- 19011 68th Ave S
The Next Generation of Dental Services
Our services are uniquely designed to reduce caregiver stress and improve patient health outcomes. We provide personalized, high-tech dental care in the comfort of the patient’s residence.

Regular dental exams are a critical part of preventive health care. During a dental exam, the dentist or hygienist will clean your teeth and check for cavities and gum disease.
Teeth cleaning is a procedure for the removal of tartar that may develop even with careful brushing and flossing, especially in areas that are difficult to reach in routine toothbrushing.
A denture is a removable replacement for missing teeth and surrounding tissues. Two types of dentures are available – complete and partial dentures.
Fillings typically used to treat cavities, as well as to repair cracked or broken teeth and teeth that have been worn down. A dentist will remove the decayed portion of the tooth and then “fill” the area where material was removed.
X-rays help the Dentist diagnose accurately and allow them to see things that they may not be able to see with the naked eye.
A dental crown is a tooth-shaped “cap” that is placed over a tooth – to cover the tooth to restore its shape and size, strength, and improve its appearance. A crown fully encases the entire visible portion of a tooth.
A dental bridge typically consists of two crowns placed on abutment teeth or implants on either side of a gap in the mouth, in addition to a pontic that joins the two crowns and fills the gap.
There are a number of reasons why tooth extraction may be necessary. It typically involves a tooth that is too badly damaged by trauma or decay to be repaired.
Root canal therapy is a treatment used to repair and save a tooth that is badly decayed or infected. It is usually performed when the nerves or blood vessels in the tooth become damaged.
A night guard is a plastic dental appliance that fits over the top teeth. Without a night guard, enamel can be worn down excessively, leading to tooth sensitivity.
Daily brushing and cleaning between your teeth is important because it removes plaque. If the plaque isn’t removed, it continues to build up, causing tooth decay and gum disease.
We pride ourselves in being able to bring the dentist office to you. We are able to do most treatments that are performed in a traditional office, but now it will be in the comfort of your own home.
Get to know our amazing dentists
We solve important dental issues and reduce stress for patients and their loved ones. Our licensed professionals are highly qualified and committed to providing the best care to our patients.

What makes them love us?
The dental cleaning was excellent, and I appreciated the email reminders about the appointment as well as the follow-up to take care of all the paperwork. This is an exceptional service, especially for the elderly who have difficulty making it to appointments when they cannot drive. I am grateful and thankful for this service!
Corey scheduled our 1st appt. by phone. He listened to my concerns & answered all of my questions. Mary & Dr.Sowle were amazing! While my daughter apologized for not taking good care of her teeth, Mary focused on what she was doing right! They make a great team. Very patient focused and friendly. Thank you for this much needed service!
They came out to see Mom for a dental problem she’s 95 and cannot walk. I didn’t know what I was going to do about the dental issue and was so relieved to find this service. I was very impressed with Enable Dental and their staff. Now we’re going to set up regular visits for dental care.
Texas Mobile Dentist has been an absolute joy to work with at Sundance Memory Care. I really consider them family with how well they relate and communicate with our loved ones. They are a true blessing!
Enable Dental comes to our community and provides excellent service to our dementia residents, right in their suites. I would recommend Enable Dental!
My brother John is in assisted living and having the mobile dentists come to him is so nice. He feels safer in his environment and the dentists and assistants have been so patient with him.
My mother is an assisted living residential home. Her condition poses a few challenges to transfer and transport her to medical appointments. However, this week an Enable Dental dentist made a visit to her home to perform dental work. They were extremely professional, helpful, and friendly in coordinating care. Making such a pleasant dental experience for mom.
" * " indicates required fields
Get in touch and book your first appointment
Ready to get started with Enable Dental? Book an appointment with a local Dental professional or contact our team for more information.

- Open access
- Published: 06 December 2021
Effects of home visits on quality of life among older adults: a systematic review protocol
- Yea Lu Tay ORCID: orcid.org/0000-0002-0150-2075 1 ,
- Nurul Salwana Abu Bakar 1 ,
- Ruzimah Tumiran 1 ,
- Noor Hasidah Ab Rahman 1 ,
- Noor Areefa Ameera Mohd Ma’amor 2 ,
- Weng Keong Yau 3 &
- Zalilah Abdullah 1
Systematic Reviews volume 10 , Article number: 307 ( 2021 ) Cite this article
7305 Accesses
3 Citations
6 Altmetric
Metrics details
Home visiting services for older adults have been offered for decades to maintain and promote health and independent functioning, thus enhancing quality of life. Previous systematic reviews have provided a mixed picture of the benefits of home visiting programmes in older adults, primarily because of heterogeneity in study designs, targeted populations, and intervention strategies. These reviews may also become out of date; thus, an updated synthesis of relevant studies is warranted. Our objective is to perform a systematic review of recently published primary studies on the effectiveness of multi-professional home visits on quality of life among older adults.
We will perform a comprehensive search for studies investigating the effect of a multi-professional home visit approach on quality of life among older adults. We will conduct the literature search in selected electronic databases and relevant research websites from January 2010 onwards. We will include randomised controlled trials (RCTs), cluster randomised controlled trials (cluster RCTs), and observational studies that enrolled older adults without dementia over 60 years old, along with studies involving multi-professional preventive–promotive home visit approaches not related to recent hospital discharge. We will report our planned review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We will retrieve and record relevant data in a standardised data extraction form and evaluate the quality of the included articles using the Cochrane risk of bias tool and the quality assessment tool for studies with diverse designs (QATSDD). Where appropriate, outcomes will be pooled for meta-analysis using a random-effects model. The main outcomes include quality of life, incidence of falls, depression, dementia, and emergency department admissions.
This review may provide evidence for the effectiveness of home visits in improving older adults’ quality of life. It will potentially benefit health care professionals, policymakers, and researchers by facilitating the design and delivery of interventions related to older generations and improve service delivery in future.
Systematic review registration
PROSPERO CRD42021234531 .
Peer Review reports
Population ageing is a global phenomenon. Most individuals expect to live into their sixties and beyond. The world population of adults aged 60 years and over is expected to nearly double from 12 to 22% between 2015 and 2050 [ 1 ]. In Malaysia, 20% of the total population will be over 65 years old by 2030 [ 2 ]. A recent study indicated that the life expectancy of Malaysian older adults aged 65 years was 79.8 and 82.1 years for males and females, respectively [ 3 ]. Despite the national census statistics defining older adults as those over the age of 65, Malaysia adopted the United Nations’ definition, classifying older adults as those aged 60 years and above for policy development regarding the older adult population [ 4 ]. The older adult population has a multitude of health needs and challenges, along with a deteriorating quality of life (QoL) [ 5 ].
According to the World Health Organization (WHO), QoL refers to “an individual’s perception of life in the context of the culture and value system in which he or she lives and in relation to his or her goals, expectations, standards, and concerns” [ 6 ]. QoL linked to health concepts is defined as the value assigned to the duration of life, modulated by limitations, functional status, perceptions, and social opportunities, which are influenced by diseases, injuries, treatments, and health policies [ 7 ]. QoL is increasingly recognised as a focus for healthcare service delivery in the older adult population. It allows the healthcare providers and policymakers to measure the efficacy of health interventions and evaluate multi-sectoral public policies, which include health, social, community, and policy actions [ 8 ].
Numerous healthcare interventions have been designed and implemented with the goal of maintaining or improving QoL among older adults, and most studies indicate the importance of active ageing. These studies have demonstrated that QoL among older adults can be enhanced through low-cost interventions, such as physical exercise [ 9 , 10 , 11 ]. Besides, older adults utilising the home visiting services were shown to have a better QoL outcome [ 12 , 13 ].
Home visits are defined as visits to an individual’s home by professionals, which may include nurses, social workers, physicians, physiotherapists, occupational therapists, pharmacists and other specialists [ 14 ]. There are five types of home visiting services: palliative, rehabilitative, long-term maintenance, therapeutic, and preventive–promotive home visits [ 15 ]. Preventive–promotive home visiting services have been offered for decades with the goal of maintaining and promoting the health and independent functioning of older adults. In addition, these services aim to reduce admission to hospitals or nursing homes and the associated economic burden [ 16 , 17 ].
Home visits allow health professionals to evaluate possible problems in the living environment of homebound older adults, assess their physical and mental health status, provide older adults with professional support, and refer them to specialist care if needed [ 17 ]. By reducing the risk of functional deterioration, these strategies are primarily structured to enhance the health-related QoL (HRQoL) of older adults, increase the possibility of continued independent living, and delay mortality [ 18 ].
Home visits have been shown to positively affect patient care and provider attitudes as well as increased satisfaction among homebound older adults and providers [ 19 ]. A previous study demonstrated that preventive home visits may have positive effects on QoL of older adults [ 20 ]. However, the variability in the study designs, participants, and outcome measures has made comparisons difficult. Liimata et al. (2019) conducted a randomised controlled trial (RCT) measuring the effects of preventative multidisciplinary home visits on HRQoL of older adults living independently. The team, which consisted of a nurse, a physiotherapist, and a social worker, observed a significantly slower decline of HRQoL in the intervention group, but this effect diminished after the visits ended [ 20 ]. In a separate publication from the same study, preventive home visits resulted in an improved HRQoL without incurring additional healthcare costs [ 21 ]. An effective prevention method aids in supporting quality of life among older adults. In a review on preventive home visits for older adults, Mayo-Wilson et al. (2014) analysed 64 RCTs involving older adults without dementia from database inception until December 2012. The study yielded high-quality evidence for decreasing falls but low-quality evidence for quality of life [ 22 ]. Thus, although an RCT demonstrated promising results on home visits, a review of multiple RCTs failed to observe significant results. In addition, although multi-professional preventive home visit approaches with thorough evaluation and collaboration among healthcare professionals may be more beneficial than home visits by a single professional, few studies have focused on this multi-professional preventive home visit approach [ 20 , 23 , 24 ].
Multi-professional preventive home visit interventions involve coordination between several health care professionals towards shared goals. Effective communication among the team members is crucial when the members work within the boundaries of their expertise and subsequently discuss progress in group sessions [ 25 ]. Previous systematic reviews have provided a mixed picture of the benefits of multi-professional home visiting services for older adults. Stuck et al. [ 26 ] and Touringy et al. [ 14 ] suggested that the multi-professional approach with follow-up visits was effective in identifying the needs of the older adult population. However, Mayo-Wilson et al. [ 22 ] demonstrated the challenges of concluding that preventive home visits result in reliable benefits, primarily due to variability in the study designs, participants, and intervention strategies of the preventive home visits approach.
In Malaysia, home visiting services for the older adult population are delivered by a multidisciplinary team and are primarily provided by the Ministry of Health [ 27 ]. The home visiting services offered in Malaysia include home-based treatment, pharmacy counselling, rehabilitation, and palliative services, which aim to ensure continuity of care at home, reduce hospital readmission, and improve QoL [ 28 , 29 ]. According to the National Health and Morbidity Survey (NHMS) 2018, a national community survey for elderly health in Malaysia, 28.6% of older adults perceived themselves as having poor QoL, 14.1% reported having at least one fall in the 12 months prior to the survey, 8.5% were diagnosed with dementia, and 11.2% were at risk of experiencing depressive symptoms [ 30 ]. Poor QoL in Malaysian older adults was found to be associated with lower education, depression, food insecurity, reduced functional status, and a lack of social support [ 31 ]. Hence, we seek to examine preventive–promotive strategies that specifically prevent or reduce the risk of developing dementia, depression, and falls, with the ultimate aim of improving QoL among the older adult population.
To our knowledge, the most recent systematic review of primary studies examining the multi-professional preventive home visit approach for older adults included studies conducted up to December 2012 [ 22 ]. Because the older adult population is rapidly growing, the number of studies describing the home visit intervention is increasing, and the methodological and reporting quality of these studies is improving. Hence, a comprehensive systematic review which includes recent studies is needed to provide new evidence on the effectiveness of multi-professional preventive–promotive home visits in improving QoL among older adults. This review may serve as a guideline for the healthcare professionals, policymakers, researchers, and institutions in designing and delivering interventions for older adults in future. Aligning health systems with the needs of the older adult population may help to promote healthy ageing in Malaysia in the long term.
This study aims to systematically assess the effect of a multi-professional home visit approach on QoL among older adults.
The present protocol has been registered within the PROSPERO database (registration number CRD42021234531) and is being reported in accordance with the reporting guidance provided in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) statement [ 32 , 33 ] (see checklist in Additional file 1).
Eligibility criteria
Types of studies.
Randomised controlled trials (RCTs), cluster randomised controlled trials (cluster RCTs), and observational studies (such as cohort, case-control, and cross-sectional studies) will be included. Quasi-randomised controlled trials (quasi-RCTs), which are often associated with a high risk of bias, and cross-over studies will be excluded. Case reports, guidelines, protocols, and short communication will also be excluded.
We will only include studies examining the older adults without dementia aged 60 years and above who reside in their own homes and receive treatment at primary care outpatient departments. We will exclude studies that involve older adults living in retirement homes or nursing homes.
Types of interventions
We will include studies that aim specifically to assess the following interventions:
Home visits which aim to prevent or reduce risks related to ageing
Home visits which utilise at least two of the following multidimensional approaches: medical, functional, psychosocial, and environmental evaluation of problems and resources, resulting in specific recommendations for solving observed problems and preventing new ones.
Types of outcome measures
Primary outcomes.
We will measure QoL using validated scales such as the WHO QoL Questionnaires, WHOQoL-BREF [ 34 ] and WHOQoL-OLD [ 35 ], the 19-item Control, Autonomy, Self-Realisation and Pleasure (CASP-19) questionnaire [ 36 ], the Older People’s Quality of Life (OPQoL) questionnaire [ 37 ], and the 36-item Short Form Health Survey (SF-36) [ 38 , 39 ].
Secondary outcomes
We will also analyse the effects of home visit interventions on the incidence of falls, depression, dementia, and emergency department admissions.
Exclusion criteria
We will exclude studies that involve follow-up visits for recent hospital discharge and studies targeting people with one specific illness.
Information sources
A comprehensive systematic electronic search will be conducted using these databases: PubMed, Ovid MEDLINE (R), the Cochrane Library, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Web of Science, ClinicalTrials.gov , the metaRegister of Controlled Trials, the Turning Research into Practice (TRIP) database, Open Grey, High Wire, the National Institute for Health and Care Excellence (NICE), and the National Institutes of Health (NIH). The search will be limited to English language articles published from January 2010 onwards.
In addition, cross-referencing will be performed, whereby the reference lists of articles will be scanned for relevant studies. We will hand-search Malaysian quality initiative or health systems project reports in the libraries of the Institute for Medical Research (IMR), Institute for Health Management (IHM), Institute for Health System Research (IHSR), Institute for Public Health (IPH), and Ministry of Health, Malaysia.
Search strategy
The search strategy will be based on the key components of the research question: population, interventions, and outcomes. It will include a mix of medical subject headings (MeSH) terms and free-text terms in the title and abstract search fields of the databases. The keywords will be related to the participants (e.g., aged, senior, older, elder, and geriatric), home care (e.g., house calls, home visits, and home care), and the outcomes (e.g., quality of life and accidental falls). Examples of the search strategy are presented in Additional file 2.
Selection of studies
Two review authors will examine the titles and abstracts independently and will exclude all irrelevant studies. Two review authors will independently retrieve and screen the full text of potentially relevant articles and identify those that meet the eligibility criteria. These steps will be recorded in an Excel table along with the reasons for study exclusion. To avoid duplication, data will be identified from the main source. Any disagreements that arise will be resolved through discussions with a third author. A PRISMA flow chart showing details of studies included and excluded at each stage of the study selection process will be provided [ 33 ].
Data extraction
Two reviewers will independently retrieve and record data in a data extraction form. Any disagreements will be resolved through discussion with the third reviewer. The data extraction form will include the following variables:
General information: title, first author, publication year, and country
Methods: study design, study duration, sample size, and mean age of the sample
Types of intervention: visitors’ professional group, number of visits, length of visits
Outcome measures:
○ Primary outcome: QoL (characteristics of the scales used to measure QoL)
○ Secondary outcomes: incidence of falls, depression, dementia, and emergency department admissions
Quality assessment
Two reviewers will evaluate the possible risk of bias for each study independently. Any disagreements will be discussed with the third reviewer. We will evaluate the RCT and cluster RCT articles for the methodological quality using the Cochrane risk of bias tool (RoB 2.0) [ 40 ]. We will categorise the risk of bias as low, high, or unclear in each of the following domains: allocation concealment, random sequence generation, blinding of outcome assessment, selective outcome reporting, incomplete outcome data, and other sources of bias.
The quality assessment tool for studies with diverse designs (QATSDD) [ 41 , 42 ] will be utilised to assess mixed-method studies. There are 14 QATSDD evaluative indicators for quantitative studies. Each indicator will be measured on a 4-point Likert scale as follows: 0 (not at all), 1 (very slightly), 2 (moderate), and 3 (complete). The maximum score of this tool is 42. The quality of a study is rated as ‘high’ if the score is over 75%, ‘good’ if it is between 50 and 75%, ‘moderate’ if it is between 25 and 50%, and ‘poor’ if it is below 25%.
Data synthesis and analysis
If the studies are sufficiently homogenous in terms of population, interventions, and outcomes, the results will be pooled, and a meta-analysis using a random-effects model will be conducted. Where possible, dichotomous data will be presented as relative risks (RRs) with 95% confidence intervals (CIs). Continuous data will be expressed as mean differences (MDs) or standardised mean differences (SMDs) (when the outcome is measured using several scales or instruments) with 95% CIs [ 43 ]. If the study characteristics are substantially different, the results will be analysed in the following subgroups, if data are available:
Participant’s age: 60–79, ≥80
Visitors’ professional group
We will interpret the heterogeneity and variability of the included studies in relation to population, interventions, outcomes, and methods. When meta-analysis is attempted, heterogeneity will be evaluated by forest plots to assess whether the CIs overlap. In addition, heterogeneity among the included studies will be measured using the chi-square ( χ 2 ) test and I 2 statistic. A small p value ( p < 0.1) for the χ 2 test and an I 2 of 50% or higher indicate moderate to substantial heterogeneity [ 44 ].
If meta-analysis is not possible, a narrative will be developed to summarise differences. We will present the data in a summary table outlining the content of the included primary studies (the number of participants, study population, description of interventions), as well as the results, conclusions, and quality ranking of studies.
Meta-bias(es)
We will assess publication bias using the Tandem method. If possible, the potential for reporting bias will be further explored using a funnel plot. A linear regression test will be performed to examine the degree of publication bias. Publication bias is significant if the p-value is less than 0.1.
Confidence in cumulative evidence
The quality of the evidence synthesised in this review will be assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology [ 45 ]. This methodology involves the evaluation of the evidence quality for each outcome across the domains of risk of bias, consistency, directness of evidence, precision of effect estimates, and publication bias, resulting in the following grades for each outcome: high, moderate, low, or very low [ 17 , 46 ].
This review may serve as evidence to support effective interdisciplinary home visits that can improve health-related QoL among older adults. This will potentially benefit policymakers and healthcare managers in planning for an efficient resource utilisation and evidence-based policy designs catered to older adults’ health. Healthcare professionals and implementers will be able to deliver health programmes and interventions suited to the needs of the older adult population. Researchers and other institutions will gain knowledge of multiple health interventions. In addition, recognising international practices will provide information to policymakers regarding strategies to improve quality of care in future.
This review has potential limitations. Our search strategy may miss sources of information available in languages other than the English language. In addition, we anticipate that the review will face challenges due to the heterogeneous nature of the study design, particularly in interventions and outcomes measures, which may limit the interpretability and comparability of results.
Protocol amendments
Any amendments to this protocol in the carrying out of this systematic review will be documented and reported in both the PROSPERO register and any subsequent publications.
Dissemination plans
The findings of this systematic review will be disseminated through publication in peer-reviewed journals and via relevant conferences. In addition, the results will also be shared with potential stakeholders, such as the Ministry of Women, Family and Community Development and the Family Health Development Division under the Ministry of Health Malaysia.
Availability of data and materials
Not applicable.
Abbreviations
Confidence interval
Cluster randomised controlled trials
Health-related quality of life
Medical subject headings
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Quality assessment tool for studies with diverse design
Quality of life
Quasi-randomised controlled trials
Randomised controlled trials
World Health Organization
World Health Organization. Ageing and health. https://www.who.int/news-room/fact-sheets/detail/ageing-and-health . Accessed 26 Aug 2021.
Institute for Public Health Malaysia. National Health and Morbidity Survey 2018 (NHMS 2018): Elderly health. Vol. I: methodology and general findings. Selangor: Institute for Public Health, National Institutes of Health, Ministry of Health Malaysia; 2019. http://iku.moh.gov.my/images/IKU/Document/REPORT/NHMS2018/NHMS2018ElderlyHealthVolume1.pdf . Accessed 10 Oct 2020
Google Scholar
Department of Statistics Malaysia. Abridged life tables, Malaysia, 2017-2019. https://www.dosm.gov.my/v1/index.php?r=column/pdfPrev&id=YnV4S1FyVnNzUWJlQ3F5NHVMeFY3UT09 . Accessed 10 Oct 2020.
Sooryanarayana R, Sazlina S-G. The Malaysian National Health and Morbidity Survey (NHMS) 2018: older persons’ health in Malaysia. Geriatr Gerontol Int. 2020;20(S2):5–6.
Article PubMed Google Scholar
Borglin G, Edberg A-K, Rahm Hallberg I. The experience of quality of life among older people. J Aging Stud. 2005;19(2):201–20.
Article Google Scholar
World Health Organization. WHOQOL-BREF: introduction, administration, scoring and generic version of the assessment. Geneva: Programme on Mental Health, World Health Organization; 1996. http://www.who.int/mental_health/media/en/76.pdf . Accessed 5 Oct 2020
Patrick DL, Erickson P. Health status and health policy: quality of life in health care evaluation and resource allocation. New York: Oxford University Press; 1993.
Institute for Public Health Malaysia. National Health and Morbidity Survey 2018 (NHMS 2018): Elderly health. Vol. II: elderly health findings. Selangor: Institute for Public Health, National Institutes of Health, Ministry of Health Malaysia; 2019. http://iku.moh.gov.my/images/IKU/Document/REPORT/NHMS2018/NHMS2018ElderlyHealthVolume2.pdf . Accessed 18 Oct 2020
Van Malderen L, Mets T, Gorus E. Interventions to enhance the quality of life of older people in residential long-term care: a systematic review. Ageing Res Rev. 2013;12(1):141–50.
Gusi N, Reyes MC, Gonzalez-Guerrero JL, Herrera E, Garcia JM. Cost-utility of a walking programme for moderately depressed, obese, or overweight elderly women in primary care: a randomised controlled trial. BMC Public Health. 2008;8:231.
Article PubMed PubMed Central Google Scholar
Eyigor S, Karapolat H, Durmaz B. Effects of a group-based exercise program on the physical performance, muscle strength and quality of life in older women. Arch Gerontol Geriatr. 2007;45(3):259–71.
Han SJ, Kim HK, Storfjell J, Kim MJ. Clinical outcomes and quality of life of home health care patients. Asian Nurs Res. 2013;7(2):53–60.
Bökberg C, Ahlström G, Karlsson S. Significance of quality of care for quality of life in persons with dementia at risk of nursing home admission: a cross-sectional study. BMC Nurs. 2017;16:39.
Tourigny A, Bédard A, Laurin D, Kröger E, Durand P, Bonin L, et al. Preventive home visits for older people: a systematic review. Can J Aging. 2015;34(4):506–23.
Elkan R, Kendrick D. What is the effectiveness of home visiting or homebased support for older people? Copenhagen: WHO Regional Office for Europe; 2004. http://www.euro.who.int/Document/e83105.pdf . Accessed 14 Sept 2020
Tøien M, Heggelund M, Fagerström L. How do older persons understand the purpose and relevance of preventive home visits? A study of experiences after a first visit. Nurs Res Pract. 2014;2014:640583.
PubMed PubMed Central Google Scholar
Grant S, Parsons A, Burton J, Montgomery P, Underhill K, Wilson EM. Home visits for prevention of impairment and death in older adults: a systematic review. Campbell Syst Rev. 2014;10(1):1–85.
Bannenberg N, Førland O, Iversen T, Karlsson M, Øien H. Preventive home visits. CINCH Working Paper Series 2019;1907:52.
Goroncy A, Makaroff K, Trybula M, Regan S, Pallerla H, Goodnow K, et al. Home visits improve attitudes and self-efficacy: a longitudinal curriculum for residents. J Am Geriatr Soc. 2020;68(4):852–8.
Liimatta H, Lampela P, Laitinen-Parkkonen P, Pitkala KH. Effects of preventive home visits on health-related quality-of-life and mortality in home-dwelling older adults. Scand J Prim Health Care. 2019;37(1):90–7.
Liimatta HA, Lampela P, Kautiainen H, Laitinen-Parkkonen P, Pitkala KH. The effects of preventive home visits on older people’s use of health care and social services and related costs. J Gerontol A Biol Sci Med Sci. 2020;75(8):1586–93.
Mayo-Wilson E, Grant S, Burton J, Parsons A, Underhill K, Montgomery P. Preventive home visits for mortality, morbidity, and institutionalization in older adults: a systematic review and meta-analysis. PLoS One. 2014;9(3):e89257.
Sommers LS, Marton KI, Barbaccia JC, J. R. Physician, nurse, and social worker collaboration in primary care for chronically ill seniors. Arch Intern Med. 2000;160(12):1825–33.
Article CAS PubMed Google Scholar
Counsell SR, Callahan CM, Clark DO, Tu W, Buttar AB, Stump TE, et al. Geriatric care management for low-income seniors: a randomized controlled trial. JAMA. 2007;298(22):2623–33.
Seiger Cronfalk B, Fjell A, Carstens N, Rosseland LMK, Rongve A, Rönnevik DH, et al. Health team for the elderly: a feasibility study for preventive home visits. Prim Health Care Res Dev. 2017;18(3):242–52.
Stuck AE, Egger M, Hammer A, Minder CE, Beck JC. Home visits to prevent nursing home admission and functional decline in elderly people: systematic review and meta-regression analysis. JAMA. 2002;287(8):1022–8.
Institute for Health Systems Research Malaysia. National Health and Morbidity Survey (NHMS) 2019: Vol. II: healthcare demand. Selangor: Institute for Health Systems Research, National Institutes of Health, Ministry of Health Malaysia; 2020. https://ihsr.moh.gov.my/images/publication_material/NHMS2019/hcd2019_report.pdf . Accessed 26 Aug 2021
Ismail NR, Abdul Hamid A, Hamid NA. Domiciliary care service: factors influencing improvement in activities of daily living among stroke survivors. Home Health Care Manag Pract. 2019;32(1):45–52.
Sivalingam N, Lim RBL, Rampal L. Palliative care in Malaysia: the need to do much more. Med J Malaysia. 2021;76(3):279–83.
CAS PubMed Google Scholar
Sooryanarayana R, Wong NI, Ahmad NA, Razak MAA, Yusoff MFM, Chan YY, et al. An overview of the methodology and general findings from the National Health and Morbidity Survey (NHMS) 2018: older persons’ health in Malaysia. Geriatr Gerontol Int. 2020;20(S2):7–15.
Abdul Mutalip MH, Abdul Rahim FA, Mohamed Haris H, Yoep N, Mahmud AF, Salleh R, et al. Quality of life and its associated factors among older persons in Malaysia. Geriatr Gerontol Int. 2020;20(S2):92–7.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Skevington S, Lotfy M, O'Connell K, WHOQOL Group. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004;13(2):299–310.
Power M, Quinn K, Schmidt S. Development of the WHOQOL-old module. Qual Life Res. 2005;14(10):2197–214.
Hyde M, Wiggins R, Higgs P, Blane D. A measure of quality of life in early old age: the theory, development and properties of a needs satisfaction model (CASP-19). Aging Ment Health. 2003;7(3):186–94.
Bowling A. The psychometric properties of the older people's quality of life questionnaire, compared with the CASP-19 and the WHOQOL-OLD. Curr Gerontol Geriatr Res. 2009;2009:298950.
Ware JE, Robert HB, Allyson RD, Kathleen NW, Anita S, William HR, et al. Conceptualization and measurement of health for adults in the health insurance study: Vol. I: model of health and methodology. Santa Monica: RAND Corporation; 1980. https://www.rand.org/pubs/reports/R1987z1.html . Accessed 17 Sept 2020
Burholt V, Nash P. Short Form 36 (SF-36) health survey questionnaire: normative data for Wales. J Public Health. 2011;33(4):587–603.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
Sirriyeh R, Lawton R, Gardner P, Armitage G. Reviewing studies with diverse designs: the development and evaluation of a new tool. J Eval Clin Pract. 2012;18(4):746–52.
Fenton L, Lauckner H, Gilbert R. The QATSDD: comments and critiques. J Eval Clin Pract. 2015;21:1125–8.
Murad MH, Wang Z, Chu H, Lin L. When continuous outcomes are measured using different scales: guide for meta-analysis and interpretation. BMJ. 2019;364:k4817.
Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Guyatt GH, Oxman AD, Schünemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. 2011;64(4):380–2.
Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;349:g7647.
Download references
Acknowledgements
We would like to express our appreciation to the Director General of Health Malaysia for his permission to publish this systematic review protocol. We would also like to thank the Director of the Institute for Health Systems Research, National Institutes of Health Malaysia for her permission to conduct this review.
The authors declare that they have received no specific funding for this work.
Author information
Authors and affiliations.
Institute for Health Systems Research, National Institutes of Health, Ministry of Health Malaysia, 40170, Shah Alam, Selangor, Malaysia
Yea Lu Tay, Nurul Salwana Abu Bakar, Ruzimah Tumiran, Noor Hasidah Ab Rahman & Zalilah Abdullah
Institute of Biological Sciences, Faculty of Science, Universiti Malaya, 50603, Kuala Lumpur, Malaysia
Noor Areefa Ameera Mohd Ma’amor
General Medical Department, Hospital Kuala Lumpur, Ministry of Health Malaysia, Jalan Pahang, 50586, Kuala Lumpur, Malaysia
Weng Keong Yau
You can also search for this author in PubMed Google Scholar
Contributions
Conceiving the protocol: YLT, NSAB, and ZA. Designing the protocol: YLT and NSAB. Coordinating the protocol: ZA. Designing search strategies: YLT, NSAB, and NAAMM. Writing the protocol: YLT, NSAB, RT, NHAR, and ZA. Providing general advice on the protocol: WKY. The authors read and approved the final manuscript.
Corresponding author
Correspondence to Yea Lu Tay .
Ethics declarations
Ethics approval and consent to participate.
This systematic review protocol was registered with the National Medical Research Register (NMRR-20-1810-56054), Ministry of Health Malaysia. Ethical approval was sought from the Health Medical Research Ethics Committee (MREC), Ministry of Health Malaysia, on 9 September 2020.
Consent for publication
Competing interests.
The authors declare that they have no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1:..
PRISMA 2020 Checklist
Additional file 2:.
Rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Tay, Y.L., Abu Bakar, N.S., Tumiran, R. et al. Effects of home visits on quality of life among older adults: a systematic review protocol. Syst Rev 10 , 307 (2021). https://doi.org/10.1186/s13643-021-01862-8
Download citation
Received : 05 February 2021
Accepted : 19 November 2021
Published : 06 December 2021
DOI : https://doi.org/10.1186/s13643-021-01862-8
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Systematic review
- Meta-analysis
- House calls
- Home visits
Systematic Reviews
ISSN: 2046-4053
- Submission enquiries: Access here and click Contact Us
- General enquiries: [email protected]
Status message
Moscow office.
1350 Troy Highway Moscow , ID 83843 United States
COMMENTS
Home health care services may be available to help older people with many aspects of health care, such as medications, wound care, medical equipment, and physical therapy. The provider may come for a few hours each day or stay 24/7. Home health care services may include in-home nursing care to help a person recover from surgery, an accident, or ...
Across the care industry, home visits are an increasingly popular choice for elderly care - helping older people to live and independent life and stay in the comfort of their own homes. A home care visit is when a professional carer comes to your home, often for between 30minutes to a few hours a day, to provide support with day to day tasks.
Contact your nearest home care office or call 800-365-4189 with your senior home care questions. Visiting Angels will conduct a free, no obligation home care assessmentand then identify a professional caregiver who has the skills, personality, and availability to assist. You will be able to meet the caregiver before they begin working for you.
House call doctor visits benefit older adults and caregivers. Getting your older adult to the doctor's office for an appointment can be difficult or sometimes impossible. Whether they're frail, can't walk on their own, or have Alzheimer'sor dementia, getting out of the house is hard on both of you.
Washington, D.C., Neighborhood. To learn more about our services in the Washington, D.C., region, call us today at 202-877-0570. The MedStar Health MedStar House Call Program - MedStar Total Elder Care is nationally recognized and offers house calls by doctors, nurse practitioners and provides diagnostic tests and treatments.
The median annual cost for a home health aide is $61,776, or $27 per hour. Most in-home care companies charge by the hour, with a typical range between $20 and $40, depending on the market. Each ...
We accept Medicare, many insurance plans, and self-pay. To find out more about our services: Call Toll-free: (855) 232-0644. E-mail us at. [email protected]. Primary Care. Psychiatry. Wound Care. Pain Management.
Federal, state, and local governments offer many resources for older adults and their families and caregivers. A good place to start is the Eldercare Locator, which connects older Americans and their caregivers with trustworthy local support resources. Visit the Eldercare Locator or call 800-677-1116.
In the U.S. Eldercare Locator - A national searchable database of community resources for elder care, from transportation to meals and home care. You can also call 1-800-677-1116. (US Department of Health and Human Services) UK. Help at Home - A guide to understanding how to get care and support for seniors in the UK.
Visiting Angels is a name families can trust to provide the best home care for their loved ones. We have been a leading elder care provider since 1998. Our professional and dedicated caregivers proudly help older adults live comfortably, independently, and safely in their own homes. Contact us today to schedule a free in-home assessment and ...
Home visits allow health professionals to evaluate possible problems in the living environment of homebound ... 2018, a national community survey for elderly health in Malaysia, 28.6% of older adults perceived themselves as having poor QoL, 14.1% reported having at least one fall in the 12 months prior to the survey, 8.5% were ...
Home visits are used for a variety of services and patient populations. ... and to support aging in place for the elderly. 5, 6, 20, 21 Interviewed ACOs reported using home visits for each of ...
Friend to Friend America recruits and matches volunteers to visit (one-to-one) with elderly and disabled persons who live in nursing, assisted living, retirement, and adult family homes to form friendships. The volunteer friends commit to visiting at least twice a month at their convenience for a minimum of one year.
As a geriatric social worker I have made many home-visits with Dr. Kauffman. My clients (some are bed bound) are sometimes nervous thinking about how a visit could be done by a dentist in the home. From the minute she walks into the bedroom and gives the biggest hello, my clients smile back and I can see they become relaxed and happy and ...
Covered home health services include: Medically necessary. part-time or intermittent skilled nursing care. Part-time or intermittent skilled nursing care. Part-time or intermittent nursing care is skilled nursing care you need or get less than 7 days each week or less than 8 hours each day over a period of 21 days (or less) with some exceptions ...
And policy does require "An Adult Protective Services (APS) investigation is initiated by a visit to the vulnerable adult who is the alleged victim at the adult's home or other place of residence.". (340:5-5-2. Initiating investigations) The Toll-Free Hotline number for Child Abuse/Neglect and Adult Abuse/Neglect is. 1-800-522-3511.
At-home dentistry across the country. With over 20 locations across the country and 10 more opening soon, Enable Dental is ready to serve you and your community. California. 5 regions. 6500 Dublin Blvd ste 210.
Home visits have been shown to positively affect patient care and provider attitudes as well as increased satisfaction among homebound older adults and providers . A previous study demonstrated that preventive home visits may have positive effects on QoL of older adults . However, the variability in the study designs, participants, and outcome ...
Arrange a time to visit the facility first, without your children. If it feels like a comfortable and inviting place, bring your children the next time. Prepare your child for the initial visit. Explain why volunteering with older adults matters—both for your family and for the elderly. Explain that some people might look ill or frail.
A BLENDED MODEL. Home visit provision is, however, a contentious issue, and who should provide these home visits also remains a moot point with a limited evidence base. 8 Paramedics and advanced nurse practioners are increasingly used for home visits in primary care in the UK, but there is wide variation. A recent systematic review reported a reduction in GP workload in some studies where ...
According to Russian government statistics, Russia had 37.3 million people over the government pension age, 60 for women and 65 for men (approximately 25 percent of the population) as of January ...
1350 Troy Highway. Moscow, ID 83843. United States. Monday - Friday: 8:00 am-5:00 pm. Saturday - Sunday: Closed. Closed on holidays. Some services are only available by phone. Please call first before going to an office. Services Phone Numbers.
Walking tour around Moscow-City.Thanks for watching!MY GEAR THAT I USEMinimalist Handheld SetupiPhone 11 128GB https://amzn.to/3zfqbboMic for Street https://...