
9.5 Types of Body Movements
Learning objectives.
By the end of this section, you will be able to:
Define and identify the different body movements
- Demonstrate the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The degree and type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints ( Table 9.1 ). Movement types are generally paired, with one directly opposing the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure 9.5.1 as you go through this section.
External Website

Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?

Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior motions are flexion and all posterior motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 9.5.1 a-d ).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 9.5.1 e ).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 9.5.1 e ).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 9.5.1 f ). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 9.5.2 g ).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 9.5.2 h ).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 9.5.2 i ).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 9.5.2 j .)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 9.5.2 k ).
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 9.5.2 l ).
Chapter Review
The variety of movements provided by the different types of synovial joints allows for a large range of body motions and gives you tremendous mobility. These movements allow you to flex or extend your body or limbs, medially rotate and adduct your arms and flex your elbows to hold a heavy object against your chest, raise your arms above your head, rotate or shake your head, and bend to touch the toes (with or without bending your knees).
Each of the different structural types of synovial joints also allow for specific motions. The atlantoaxial pivot joint provides side-to-side rotation of the head, while the proximal radioulnar articulation allows for rotation of the radius during pronation and supination of the forearm. Hinge joints, such as at the knee and elbow, allow only for flexion and extension. Similarly, the hinge joint of the ankle only allows for dorsiflexion and plantar flexion of the foot.
Condyloid and saddle joints are biaxial. These allow for flexion and extension, and abduction and adduction. The sequential combination of flexion, adduction, extension, and abduction produces circumduction. Multiaxial plane joints provide for only small motions, but these can add together over several adjacent joints to produce body movement, such as inversion and eversion of the foot. Similarly, plane joints allow for flexion, extension, and lateral flexion movements of the vertebral column. The multiaxial ball and socket joints allow for flexion-extension, abduction-adduction, and circumduction. In addition, these also allow for medial (internal) and lateral (external) rotation. Ball-and-socket joints have the greatest range of motion of all synovial joints.
Interactive Link Questions
Dorsiflexion of the foot at the ankle decreases the angle of the ankle joint, while plantar flexion increases the angle of the ankle joint.
Review Questions
1. Briefly define the types of joint movements available at a ball-and-socket joint.
2. Discuss the joints involved and movements required for you to cross your arms together in front of your chest.
Answers for Critical Thinking Questions
- Ball-and-socket joints are multiaxial joints that allow for flexion and extension, abduction and adduction, circumduction, and medial and lateral rotation.
- To cross your arms, you need to use both your shoulder and elbow joints. At the shoulder, the arm would need to flex and medially rotate. At the elbow, the forearm would need to be flexed.
This work, Anatomy & Physiology, is adapted from Anatomy & Physiology by OpenStax , licensed under CC BY . This edition, with revised content and artwork, is licensed under CC BY-SA except where otherwise noted.
Images, from Anatomy & Physiology by OpenStax , are licensed under CC BY except where otherwise noted.
Access the original for free at https://openstax.org/books/anatomy-and-physiology/pages/1-introduction .
Anatomy & Physiology Copyright © 2019 by Lindsay M. Biga, Staci Bronson, Sierra Dawson, Amy Harwell, Robin Hopkins, Joel Kaufmann, Mike LeMaster, Philip Matern, Katie Morrison-Graham, Kristen Oja, Devon Quick, Jon Runyeon, OSU OERU, and OpenStax is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License , except where otherwise noted.
Module 10: Joints
Types of body movements, learning objectives.
- Define the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints (Table 1). Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward.
Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?
Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 1).

Figure 1. Flexion and extension. (a)–(b) Flexion and extension motions are in the sagittal (anterior–posterior) plane of motion. These movements take place at the shoulder, hip, elbow, knee, wrist, metacarpophalangeal, metatarsophalangeal, and interphalangeal joints. (c)–(d) Anterior bending of the head or vertebral column is flexion, while any posterior-going movement is extension.
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction, Adduction, and Circumduction

Figure 2. Abduction, adduction, and circumduction.
Abduction and adduction are motions of the limbs, hand, fingers, or toes in the coronal (medial–lateral) plane of movement. Moving the limb or hand laterally away from the body, or spreading the fingers or toes, is abduction. Adduction brings the limb or hand toward or across the midline of the body, or brings the fingers or toes together. Circumduction is the movement of the limb, hand, or fingers in a circular pattern, using the sequential combination of flexion, adduction, extension, and abduction motions.
Adduction, abduction, and circumduction take place at the shoulder, hip, wrist, metacarpophalangeal, and metatarsophalangeal joints.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 2).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 2).

Figure 3. Rotation.
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 3). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Turning of the head side to side or twisting of the body is rotation. Medial and lateral rotation of the upper limb at the shoulder or lower limb at the hip involves turning the anterior surface of the limb toward the midline of the body (medial or internal rotation) or away from the midline (lateral or external rotation).
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 4).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 4).

Figure 4. Supination and pronation. (a) Supination of the forearm turns the hand to the palm forward position in which the radius and ulna are parallel, while forearm pronation turns the hand to the palm backward position in which the radius crosses over the ulna to form an “X.” (b) Dorsiflexion of the foot at the ankle joint moves the top of the foot toward the leg, while plantar flexion lifts the heel and points the toes.
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 5).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 5.)

Figure 5. Inversion, eversion, protraction, and retraction. (a) Eversion of the foot moves the bottom (sole) of the foot away from the midline of the body, while foot inversion faces the sole toward the midline. (b) Protraction of the mandible pushes the chin forward, and retraction pulls the chin back.
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 6).

Figure 6. Depression, elevation, and opposition. (a) Depression of the mandible opens the mouth, while elevation closes it. (b) Opposition of the thumb brings the tip of the thumb into contact with the tip of the fingers of the same hand and reposition brings the thumb back next to the index finger.
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 6).
- Chapter 9. Authored by : OpenStax College. Provided by : Rice University. Located at : http://cnx.org/contents/[email protected]@7.1. . Project : Anatomy & Physiology. License : CC BY: Attribution . License Terms : Download for free at http://cnx.org/content/col11496/latest/
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
11.10 Types of Body Movements
Learning Objectives
By the end of this section, you will be able to:
- Define the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint result from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints (Table 11.10.1). Movement types are paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure 11.10.1 as you go through this section.

Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 11.10.1a-d).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 11.10.1e).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 11.10.1e).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation. Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 11.10.1f). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 11.10.2g).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 11.10.2h).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilise the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 11.10.2i).
Protraction and Reaction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 11.10.2j.)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 11.10.2k).
Excursion is the side-to-side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a particularly important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 11.10.2l).
Table 11.10.1. Movements of the Joints
Section Review
The variety of movements provided by the several types of synovial joints allows for a broad range of body motions and gives you tremendous mobility. These movements allow you to flex or extend your body or limbs, medially rotate, and adduct your arms and flex your elbows to hold a heavy object against your chest, raise your arms above your head, rotate or shake your head, and bend to touch the toes (with or without bending your knees).
Each of the different structural types of synovial joints also allow for specific motions. The atlantoaxial pivot joint provides side-to-side rotation of the head, while the proximal radioulnar articulation allows for rotation of the radius during pronation and supination of the forearm. Hinge joints, such as at the knee and elbow, allow only for flexion and extension. Similarly, the hinge joint of the ankle only allows for dorsiflexion and plantar flexion of the foot.
Condyloid and saddle joints are biaxial. These allow for flexion and extension, and abduction and adduction. The sequential combination of flexion, adduction, extension, and abduction produces circumduction. Multiaxial plane joints provide for only small motions, but these can add together over several adjacent joints to produce body movement, such as inversion and eversion of the foot. Similarly, plane joints allow for flexion, extension, and lateral flexion movements of the vertebral column. The multiaxial ball and socket joints allow for flexion-extension, abduction-adduction, and circumduction. In addition, these also allow for medial (internal) and lateral (external) rotation. Ball-and-socket joints have the greatest range of motion of all synovial joints.
Review Questions
Critical Thinking Questions
Click the drop down below to review the terms learned from this chapter.
Fundamentals of Anatomy and Physiology Copyright © 2021 by University of Southern Queensland is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License , except where otherwise noted.
Share This Book
9.5 Types of Body Movements
Learning objectives.
By the end of this section, you will be able to:
- Define the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints ( Table 9.1 ). Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure 9.12 as you go through this section.
Interactive Link
Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?
Flexion and Extension
Flexion and extension are typically movements that take place within the sagittal plane and involve anterior or posterior movements of the neck, trunk, or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or trunk, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion of the vertebral column occurs in the coronal plane and is defined as the bending of the neck or trunk toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 9.12 a-d ).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 9.12 e ).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 9.12 e ).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 9.12 f ). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 9.13 g ).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 9.13 h ).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 9.13 i ).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 9.13 j .)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 9.13 k ).
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 9.13 l ).
This book may not be used in the training of large language models or otherwise be ingested into large language models or generative AI offerings without OpenStax's permission.
Want to cite, share, or modify this book? This book uses the Creative Commons Attribution License and you must attribute OpenStax.
Access for free at https://openstax.org/books/anatomy-and-physiology-2e/pages/1-introduction
- Authors: J. Gordon Betts, Kelly A. Young, James A. Wise, Eddie Johnson, Brandon Poe, Dean H. Kruse, Oksana Korol, Jody E. Johnson, Mark Womble, Peter DeSaix
- Publisher/website: OpenStax
- Book title: Anatomy and Physiology 2e
- Publication date: Apr 20, 2022
- Location: Houston, Texas
- Book URL: https://openstax.org/books/anatomy-and-physiology-2e/pages/1-introduction
- Section URL: https://openstax.org/books/anatomy-and-physiology-2e/pages/9-5-types-of-body-movements
© Jun 13, 2024 OpenStax. Textbook content produced by OpenStax is licensed under a Creative Commons Attribution License . The OpenStax name, OpenStax logo, OpenStax book covers, OpenStax CNX name, and OpenStax CNX logo are not subject to the Creative Commons license and may not be reproduced without the prior and express written consent of Rice University.

Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
2 Types of Body Movements
Learning objectives.
By the end of this section, you will be able to:
- Define the different types of body movements
- Identify the joints that allow for these motions
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints ( Table 1 ). Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure 1 as you go through this section.

Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?

Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 1 a-d ).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 1 e ).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 1 e ).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 1 f ). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 2 g ).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 2 h ).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 2 i ).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 2 j .)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 2 k ).
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 2 l ).
Chapter Review
The variety of movements provided by the different types of synovial joints allows for a large range of body motions and gives you tremendous mobility. These movements allow you to flex or extend your body or limbs, medially rotate and adduct your arms and flex your elbows to hold a heavy object against your chest, raise your arms above your head, rotate or shake your head, and bend to touch the toes (with or without bending your knees).
Each of the different structural types of synovial joints also allow for specific motions. The atlantoaxial pivot joint provides side-to-side rotation of the head, while the proximal radioulnar articulation allows for rotation of the radius during pronation and supination of the forearm. Hinge joints, such as at the knee and elbow, allow only for flexion and extension. Similarly, the hinge joint of the ankle only allows for dorsiflexion and plantar flexion of the foot.
Condyloid and saddle joints are biaxial. These allow for flexion and extension, and abduction and adduction. The sequential combination of flexion, adduction, extension, and abduction produces circumduction. Multiaxial plane joints provide for only small motions, but these can add together over several adjacent joints to produce body movement, such as inversion and eversion of the foot. Similarly, plane joints allow for flexion, extension, and lateral flexion movements of the vertebral column. The multiaxial ball and socket joints allow for flexion-extension, abduction-adduction, and circumduction. In addition, these also allow for medial (internal) and lateral (external) rotation. Ball-and-socket joints have the greatest range of motion of all synovial joints.
Interactive Link Questions
Dorsiflexion of the foot at the ankle decreases the angle of the ankle joint, while plantar flexion increases the angle of the ankle joint.
Review Questions
1. The joints between the articular processes of adjacent vertebrae can contribute to which movement?
- lateral flexion
- circumduction
- dorsiflexion
2. Which motion moves the bottom of the foot away from the midline of the body?
- plantar flexion
3. Movement of a body region in a circular movement at a condyloid joint is what type of motion?
4. Supination is the motion that moves the ________.
- hand from the palm backward position to the palm forward position
- foot so that the bottom of the foot faces the midline of the body
- hand from the palm forward position to the palm backward position
- scapula in an upward direction
5. Movement at the shoulder joint that moves the upper limb laterally away from the body is called ________.
- lateral rotation
Critical Thinking Questions
1. Briefly define the types of joint movements available at a ball-and-socket joint.
2. Discuss the joints involved and movements required for you to cross your arms together in front of your chest.
Answers for Review Questions
Answers for Critical Thinking Questions
- Ball-and-socket joints are multiaxial joints that allow for flexion and extension, abduction and adduction, circumduction, and medial and lateral rotation.
- To cross your arms, you need to use both your shoulder and elbow joints. At the shoulder, the arm would need to flex and medially rotate. At the elbow, the forearm would need to be flexed.
Anatomical Basis of Injury Copyright © 2019 by Layci Harrison is licensed under a Creative Commons Attribution 4.0 International License , except where otherwise noted.
Share This Book
Registered Nurse RN
Registered Nurse, Free Care Plans, Free NCLEX Review, Nurse Salary, and much more. Join the nursing revolution.
Body Movement Terms – Anatomy Body Planes of Motions
In this anatomy lesson, I’m going to cover all of the major body movement terms for anatomy (also called the planes of motion ) that can occur at the synovial joints. You’ll come across these in your anatomy or kinesiology courses, and if you pursue a career in healthcare, you’ll use these terms during documentation or patient assessments.
After you review these notes and the corresponding video, you can take a comprehensive quiz on anatomy body movement terms .
Categories of Body Movement Terms in Anatomy
There are four major categories of body movements that can occur at the synovial joints:
- Gliding movement
- Angular movements
- Rotational movements
- Special movements
Gliding Movement in Anatomy
What is gliding ? Gliding occurs when the surfaces of bones slide past one another in a linear direction, but without significant rotary or angular movement.
An example of this movement is moving your hand back and forth (left to right) in a waving motion, which causes gliding to occur at the joints of the carpals ( wrist bones ). When you move your hand back and forth in a waving motion, it can help you remember that gliding joint movements primarily take place in the carpals of the wrist and the tarsals of the ankle.

However, gliding can also occur in the other plane joints (also called planar joints) of the body. Just as airplanes glide through the air, the plane joints of the body allow a gliding motion.
Other plane joints that allow gliding include the sacroiliac joint of the pelvis , the acromioclavicular joint of the shoulder, the femoropatellar joint , tibiofibular joint , sternocostal joints for ribs 2-7, vertebrocostal joints , and the intervertebral joints of the spine (at the articular processes).
Angular Movements in Anatomy
The next category of body movement terms consists of the angular movements, which consist of the following movements:
- Flexion and Extension
- Abduction and Adduction
- Circumduction
Flexion and Extension in Anatomy
Because flexion and extension are angular movements, I find it really helpful to visualize an angle during the actual movement. Flexion decreases the angle between two structures or joints as they bend or move closer together, whereas extension increases the angle between them as they straighten and move apart.
Elbow Flexion and Extension
Elbow flexion (also called forearm flexion ) occurs when the angle between the forearm and arm decreases, allowing the ulna of the forearm to move closer to the humerus bone of the arm.
In contrast, elbow extension ( forearm extension ) occurs when the forearm moves away from the arm, increasing the angle between those bones.

Shoulder Flexion and Extension
Shoulder flexion , also called arm flexion , occurs when the angle at the humerus of the arm and the scapula decreases as the arms move anteriorly. In contrast, shoulder extension (or arm extension ) occurs when the angle at the humerus of the arm and the scapula increases, causing the arm to move posteriorly. The joint here allows movement past the anatomical position. Some anatomists call arm movement beyond the anatomical position extension , whereas some call it hyperextension .

Wrist Flexion and Extension
Wrist flexion (also called hand flexion ) occurs when the angle between the palm of the hand and the anterior surface of the forearm decreases, while wrist extension (or hand extension ) is moving the palm of the hand away from the anterior surface of the forearm, hence the angle increases. This is another joint that can continue to move past the anatomical position in a posterior direction, which some anatomists call hyperextension.

Finger Flexion and Extension
Finger flexion occurs when the angle between the fingers and the palm decreases, as the fingers move toward the palm. When the angle between the fingers and the palm increases, finger extension occurs.

Flexion and extension also occur with the interphalangeal joints of the fingers (digits 2-5), including the distal interphalangeal joint (dip) and proximal interphalangeal joint (pip).

Thumb Flexion and Extension
The thumb (pollex) can confuse people because thumb flexion and extension occur in the frontal plane , which is a different direction than flexion of the fingers, which occurred in the sagittal plane. Thumb flexion moves the thumb toward the pinky finger, whereas extension moves the thumb away from the pinky finger. Think of your palm as a windshield and your thumb as the windshield wiper for this movement.

Flexion and extension can also occur at the interphalangeal joint of the thumb.

Hip Flexion and Extension
Hip flexion (or thigh flexion ) occurs when the angle between the femur of the thigh and hipbone decreases as the thigh moves anteriorly (forward). Hip extension ( thigh extension ) occurs when the angle between the femur and the hip bone increases, as the hip joint straightens. This joint also allows posterior movement past the anatomical position, which some anatomists call hyperextension.

Knee Flexion and Extension
Knee flexion ( leg flexion ) occurs when the tibia bone moves toward the femur, causing the angle to decrease between those two structures. Knee extension (or leg extension ) occurs as the angle between the leg bones increases, causing the leg to straighten.

Toe Flexion and Extension
Like the fingers, toe flexion and extension can also occur. Toe flexion involves bending the toes toward the sole of the foot, decreasing the angle between these two structures, while toe extension involves increasing the angle and straightening the toes.

Note : instead of using flexion and extension for the movement of the foot at the ankle joint, anatomists prefer to use the terms plantarflexion and dorsiflexion .
Neck Flexion and Extension
Neck flexion occurs as the angle between the head and the trunk of the body decreases as those two structures move closer together, whereas neck extension occurs as the head moves away from the trunk of the body, thus increasing the angle. The neck is another structure that can continue posteriorly, beyond the anatomical position, which some anatomists call hyperextension of the neck .

Vertebral Column Flexion and Extension
Vertebral column flexion at the trunk, (spine flexion) occurs when the angle between the trunk and the hip joint decreases. Vertebral column (spine) extension at the trunk occurs as the spine straightens and the angle between the hip joint and spine increases.

By the way, you might have noticed that most of these movements so far are occurring within (or parallel to) the sagittal plane. However, just like the thumb, flexion can also occur in the frontal (coronal) plane for the vertebral column. For example, if you bend the spine to the left or right, that’s called lateral flexion , and movement back toward the anatomical position is called lateral extension .

Note: you might want to watch our other lecture if you are unfamiliar with the different body planes .
Hyperextension
Finally, when extension of a structure moves beyond a certain point, anatomists call it hyperextension. However, anatomists differ on what constitutes hyperextension when it comes to body movement terms.

For example, some anatomists say that when the arm , neck , wrist , or thigh moves past the anatomical position in a posterior motion, it becomes hyperextension . Other anatomists only consider these movements hyperextension if the movement exceeds the normal range of motion permitted by the joint. For test-taking purposes, follow your anatomy teacher’s definition!
Abduction and Adduction in Anatomy
Unlike flexion and extension movements, which mostly take place within the sagittal plane , you’ll notice that abduction and adduction motions mostly take place within the frontal, or coronal, plane. However, the thumb is a notable exception to this rule, as it moves within the sagittal plane during abduction and adduction when in the anatomical position .
What is Abduction?
Abduction (think: ABDUCT ion) is the movement of a structure away from its midline reference point. Let the name help you out. What does “abduct” mean? When you hear on the news that a man was abducted, you know it means that someone took him away . That’s exactly what’s going on with this movement. The structure is being moved away from its midline reference point.
What is Adduction?
Adduction (think: ADD uction) occurs as the structure is ADDED back toward its midline reference point.
Let’s take a look at examples of abduction and adduction on the body.
Arm Abduction and Adduction
During arm abduction (also called shoulder abduction), the arms move away from the body’s midline. During arm adduction (or shoulder adduction), you ADD them right back toward the midline.

Finger Abduction and Adduction
Finger abduction occurs when the fingers move away from the midline reference of the hand, whereas finger adduction occurs when you add them back toward the hand’s midline reference.

When the middle finger (3rd digit), which serves as the midline reference of the hand, deviates to the away from the body, it’s called lateral abduction . When it deviates toward the body, it’s called medial abduction .

Thumb Abduction and Adduction
The thumb (pollex) is different from the fingers. Abduction of the thumb has it moving within the sagittal plane, in an anterior motion. Adduction of the thumb has it added back to the hand.

Wrist Abduction and Adduction (Ulnar Deviation & Radial Deviation)
When determining abduction and adduction of the wrist, I find that it helps to stand in the anatomical position. Abduction of the wrist has it moving away from the body’s midline, in the same direction as arm abduction. Adduction of the wrist has it going in the opposite direction, toward the body’s midline.

These movements are also referred to as radial deviation and ulnar deviation . Remember, the radius is on the thumb side, which where you check the radial pulse. So radial deviation is movement on the radial side, whereas ulnar deviation occurs on the opposite side.

Thigh Abduction and Adduction
During thigh abduction (also called hip abduction or leg abduction), the lower limb moves away from the body’s midline. During adduction of the thigh , you ADD the lower limb right back toward the body’s midline.

Toes Abduction and Adduction
When the toes move away from the midline of the foot, toe abduction occurs. Toe adduction adds them right back together.

Just like with the hand, devation of the 2nd toe away from the body’s midline is called lateral abduction , whereas movement toward the midline is called medial abduction .

Circumduction in Anatomy
The final body movement term in this category is circumduction , which is an angular movement that blends the motions of flexion , abduction , extension, and adduction to create a circular or conical motion of the attached structure.
The word circ umduction starts with the same letters as the word “ circ le,” so that will tip you off that this movement creates a circular, or conical, movement in the structure extending beyond the joint.
Circumduction Movement Demonstrated
Because circumduction is a combined movement, I find it helpful to think about the individual movements in slow motion. Looking at the shoulder joint, I’ll begin with arm flexion and then arm abduction. Next is arm extension , followed by arm adduction . When you combine those movements into one smooth motion, you can see how it forms a cone or circle.
The mnemonic “FABEA” might help you remember the order:
You could also reverse that order, but the movements have to alternate in a similar succession to create the circular motion that characterizes the circumduction movement.
Joints Capable of Circumduction
Where can circumduction occur on the body? Because it requires the motions of flexion, extension, abduction, and adduction, the joint will generally have to be capable of all four of those sequential movements. Below are examples of joints/structures that can perform the circumduction movement.
Circumduction of the Hip Joint (Thigh)

Circumduction of the Shoulder Joint (Arm)

Circumduction of the Wrist Joint (Hand)

Circumduction of the Thumb (Pollex)

Circumduction of the Fingers

Circumduction of the Toes

Circumduction of the Ankle Joint (Foot)

Circumduction of the Head

Rotation in Anatomy
The next category of the body planes of motion is rotation , which is a body movement term that describes a bone moving around a central axis.
Rotation Body Movement Term in Anatomy
When I think of the rotation body movement , I like to picture a screw turning to either the right or left, as that is similar to the rotation movement that can occur in the body.
Rotation can occur at the head/neck, vertebral column, and the ball-and-socket joints of the upper and lower limbs (shoulder joint and hip joint). Let’s take a look at these movements, starting with the head.
Head and Neck Rotation
The head can rotate laterally to either the left or right, thanks to the pivot joint between vertebrae C1 (atlas) and C2 (axis). Moving the head back toward the anatomical position is medial rotation of the head.

Trunk Rotation
The vertebral column can also rotate laterally to either the left or right. Returning the trunk back toward the anatomical position is medial rotation of the trunk.

Arm Rotation (Medial and Lateral)
The ball-and-socket joint of the shoulder allows the humerus of the arm to rotate laterally, or away from the body’s midline , which is also called external rotation. It can also rotate medially, or toward the body’s midline, which is also called internal rotation.

Thigh/Leg Rotation (Medial and Lateral)
The ball-and-socket joint of the hip allows rotation of the thigh’s femur . Like the humerus, it can rotate laterally, or away from the body’s midline, which is also called external rotation. It can also rotate medially, or toward the body’s midline, creating an internal rotation movement.

Tip for Medial vs Lateral Limb Rotation
Be sure to focus on the anterior surface of the femur or humerus when you do this movement, because that’s the focal point for determining medial vs lateral rotation.

Special Body Movement Terms in Anatomy
The final category of body movement terms include the “special movements.” These movements don’t fall neatly into the categories I’ve already listed, so they are placed in their own unique category. The special movements involve the following:
Supination and Pronation
- Dorsiflexion and Plantarflexion (also spelled plantar flexion)
Inversion and Eversion
Elevation and depression.
- Protraction and Retraction
- Protrusion, Retrusion, and Excursion
- Opposition and Reposition
Supination and pronation are special movements involving rotation of the forearm .
Supination of Forearm and Hand
During supination , the distal end of the radius bone rotates over the ulna bone in a lateral direction . Lateral rotation means it is rotating away from the body’s midline.
I like to watch the thumb during this movement, because it is on the same side as the radius (hence, the radial pulse is located below the thumb). When the thumb is rotating away from the body’s midline, supination is occurring.

Pronation of Forearm and Hand
In contrast, pronation is the opposite movement: the distal end of the radius rotates over the ulna medially, and the two bones cross. Medial rotation is toward the body’s midline. So when the thumbs point toward the middle of the body, you know that pronation has occurred.

Palm Orientation During Supination and Pronation
You can also look at the orientation of the palms. During supination, the palms will face anteriorly (forward), which is their natural orientation in the anatomical position. However, if you flex the elbow about 90 degrees, the palms would then be facing up (superiorly).

Pronation has the palms facing the opposite direction: posteriorly (toward the back) when in the anatomical position, or down (inferiorly) when the elbow flexes to around 90 degrees. This is another reason why I like to look at the thumbs during this movement. Thumbs will point away from the body’s midline during supination, and toward the body during pronation, regardless of how the elbow is flexed.

Supination vs Pronation Mnemonic
Here’s a simple mnemonic (memory trick) to help you remember pronation vs supination special movements:
At the grocery store, you pro nate to pick up your pro duce, and you sup inate to eat it for sup per.

Also, if you want to take your vitamins, you pro nate to p our, and you sup inate to take your sup plements.
Plantarflexion and Dorsiflexion
In this continued series on body movements of anatomy, I’m going to demonstrate dorsiflexion and plantarflexion (or plantar flexion), which are special movements involving the foot and ankle joint.
Dorsiflexion vs Plantarflexion
To help you understand this special movement, let’s break down the words.
Dorsal Side of the Foot (Dorsum)
Dorsal refers to the back (or upper) side of something. In my video on body cavities and membranes , I used the example of a dorsal fin of a dolphin to help you remember that dorsal refers to the backside of a surface. Your toenails are on the dorsal side of the foot, because they are on the back (or upper) side of it.
Plantar Side of Foot (Sole)
In contrast, plantar refers to the sole (or bottom) of the foot. If you’ve ever had a plantar wart, then you’ve had a wart on the sole of your foot (ouch!).
Flexion Meaning
Flexion refers to the movement that decreases the angle between two surfaces or joints, usually within the sagittal plane of the body. Now, let’s put all these words together, and you’ll be able to remember the difference between plantarflexion vs dorsiflexion .
Dorsiflexion Example

During dorsiflexion , the back (upper) side of the foot moves toward the shin, decreasing the angle between these two surfaces, leaving the toes pointing closer toward your head. When you try to walk on your heels only, you dorsiflex the foot.
Plantar Flexion (Plantarflexion) Example

During plantar flexion , the sole of the foot angles downward toward the calf, decreasing the angle between those two surfaces, leaving the toes pointing farther away from the body. When you perform calf raises in the gym or walk on your tip toes, you plantar flex the foot. If you need help remember the direction of this movement, just remember this phrase: “Plantarflexion helps you stand on your toes and walk in any direction!”
Next, I’m going to demonstrate inversion and eversion , which are special movements that cause the foot to move relative to the body’s midline.
Inversion of the Foot
During inversion , the bottom of the foot (sole) turns so that it faces toward the body’s midline, in a medial orientation. Inversion starts with the word “in,” so that’s the dead giveaway that the sole is pointing in wardly (medially).

Eversion of the Foot
During eversion , the opposition motion occurs: the bottom of the foot turns so that it faces away from the body’s midline (laterally). The word “evert” literally means to “turn outward,” which is exactly what happens during eversion!

Now lets’s examine elevation and depression, which are special body movement terms that describe motion in a superior (up) or inferior (down) direction.
Elevation in Anatomy
Elevation refers to movement of a body part in a superior direction, or moving upward. When you walk into a hotel lobby, you have to get on the elevator to go up, right? We’d also say that a mountain has a peak “elevation” of 20,000 feet. Therefore, the term is pretty self-explanatory: elevation has a structure moving up, or superiorly.
Depression in Anatomy
Depression refers to movement of a body part in an inferior direction, or moving downward. When you are depressed, you feel down in the dumps, right? Therefore, depression is easy to remember as movement in an inferior, or downward direction.
Elevation and Depression in Anatomy
In anatomy, elevation and depression most commonly describe movements of the mandible (lower jaw) or scapulae (shoulder blades) within the frontal plane . When you move your lower jaw (mandible) in a downward direction, depression occurs. When you move your mandible upward, elevation occurs.

Similarly, when you move your scapulae up, elevation of the shoulder girdle occurs. When you move them back down, depression of the shoulder girdle occurs.

Protraction and Retraction in Anatomy
Now let’s discuss protraction and retraction , which are special body movements in anatomy that most commonly involve the scapulae (shoulder blades).
Protraction Movement
Protraction moves the scapula forward (anteriorly) and toward the side of the body (laterally) in an anterolateral direction.

Retraction Movement
Retraction is the opposite movement. It causes the shoulder blades to move back (posteriorly) and toward the body’s midline (medially). This movement is known as a posteromedial movement.

Protraction and Retraction Mnemonic
Here’s a simple way to remember protraction and retraction body movements in anatomy:
- You Retract when you Reach Back !
- You P unch to P rotract! In fact, the serratus anterior muscles assist with protraction of the scapulae, and they even call this muscle the boxer’s muscle for that very reason.
Protrusion, Retrusion, and Excursion in Anatomy
In this anatomy lesson, I’m going to demonstrate protrusion, retrusion, and excursion , which are special body movement terms in anatomy that refer to forward (anterior), backward (posterior), or side to side movements.
Protrusion in Anatomy
Protrusion refers to the movement of a structure in an anterior (forward) direction. In fact, the word protrude means “projecting something forward.”
I call protrusion the kissing movement because it occurs when you pucker your lips like you’re going to give someone a kiss or stick out your tongue. Moving the mandible (lower jaw) forward is also an example of protrusion.

Retrusion in Anatomy
Retrusion is the opposite of protrusion. It refers to the movement of a structure in a posterior, or backward, direction. Putting your tongue back in your mouth, moving the lips back, or moving the mandible back are all examples of retrusion in anatomy.

Excursion in Anatomy
Finally, we have excursion , which refers to the side-to-side movement of the lower jaw (mandible). If you’ve ever heard of a character named Ernest P. Worrell, then you’ve definitely seen the excursion movement. He’s the character in those movies such as Ernest Goes to Camp, Ernest Goes to Jail, etc. When Ernest saw something nasty, he’d move his jaw back and forth and say, “Ewwww.”

Excursion can occur in either direction, and anatomists use directional terms to specify the type of excursion. When the mandible moves to either the left or right, it’s moving away from the body’s midline, so it’s called lateral excursion . When the mandible moves closer to the midline of the body, it’s called medial excursion .

Protrusion and Retrusion vs Protraction and Retraction
What about protraction and retraction ? Some anatomy textbooks will refer to the forward movement of the mandible, lips, or tongue as protraction (instead of protrusion), and the backward (posterior) movement will be called retraction (instead of retrusion). The terms are sometimes used interchangeably, so use whatever method your anatomy professor suggests (they give you the grade, not me!).
However, some anatomists today use protraction and retraction to refer almost exclusively to the scapulae, as it is a combined movement (protraction is anterolateral, and retraction is posteromedial). In contrast, protrusion and retrusion are more of an anterior/posterior movement. Then again, some anatomists prefer not to use protraction and retraction at all, even when describing shoulder blade movement.
Opposition and Reposition of the Thumb: Anatomy
Finally, I’ll demonstrate opposition and reposition , which are special movements involving the thumb.
The thumb, also known as the pollex or digit one, articulates (forms a joint) with the trapezium bone of the wrist (carpus) via a saddle joint, which is a type of synovial joint featuring interlocking convex and concave surfaces. They call it a saddle joint because, well, it kinda looks like a saddle (yee-haw, cowboy!).
Thanks to this saddle joint, the thumb can perform circumduction, flexion and extension, abduction and adduction, as well as special movements called opposition and reposition .
Opposition of the Thumb
Opposition of the thumb occurs when the tip of the thumb comes to meet (and oppose) the tip of another finger from the same hand. A super easy way to remember this is that you’ve probably heard someone say that humans have opposable thumbs. Oppos ition is the special movement of our oppos able thumbs.

In fact, think about this: when the opposition movement occurs, what happens? In the picture above, did you notice how the thumb and finger created a shape similar to the letter ‘O’? The ‘O’ stands for opposition! Now you can easily remember this motion of our opposable thumbs!
Reposition of the Thumb
Reposition is the opposite action of opposition. During reposition, the thumb and finger return to their original position.

Free Quiz and More Anatomy Videos
Take a free comprehensive quiz on body movement terms to test your knowledge, or review our anatomy body movement terms video . In addition, you might want to watch our anatomy and physiology lectures on YouTube, or check our anatomy and physiology notes .
Please Share:
- Click to print (Opens in new window)
- Click to share on Facebook (Opens in new window)
- Click to share on Twitter (Opens in new window)
- Click to share on Pinterest (Opens in new window)
- Click to share on Reddit (Opens in new window)
- Click to share on LinkedIn (Opens in new window)
- Click to share on WhatsApp (Opens in new window)
- Click to share on Pocket (Opens in new window)
- Click to share on Telegram (Opens in new window)
Disclosure and Privacy Policy
Important links, follow us on social media.
- Facebook Nursing
- Instagram Nursing
- TikTok Nurse
- Twitter Nursing
- YouTube Nursing
Copyright Notice
- Media Library
- Encyclopedia
- Universities

Unlock with Premium
- Dynamic occlusion: lateral excursion
The dynamic occlusion is the contact that teeth make during movements of the mandible - when the jaw moves side to side, forward, backward or at an angle. In dynamic occlusion, the contacts of the teeth are not points as in static occlusion, but they are described with lines.
- Dental occlusion
- Occlusal relationship
- Temporomandibular joint (TMJ)
- Joint capsule and ligaments of TMJ
- Movements of TMJ
- Static occlusion: centric occlusion
- Occlusion concepts: centric relation
- Angle's classification
- Angle's classification: Class I
- Angle’s classification: Class II, Division 1
- Angle's classification: Class II, Division 2
- Angle's classification: Class III
- Dynamic occlusion: canine guidance
- Dynamic occlussion: protrusion
- Curve of Spee
- Curve of Wilson
- Sphere of Monson
Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
12 2.2.3 Types of Body Movements
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by its structural type. While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints ( Table 1 ).
Human movements are complex. In order to describe movements we typically break down the movement and describe what is occurring at every joint. At each joint, we can break down the movement into three planes. Planes describe the direction of the movement. The sagittal plane lies vertically and divides the body into right and left parts. Forward and backward movements fall into this plane (flexion, extension). The frontal plane also lies vertically but divides the body into anterior and posterior parts. Lateral movements that involves the limbs moving away and towards the body fall under this plane (adduction, abduction). The transverse plane lies horizontally and divides the body into superior and inferior. Rotations and twisting motions fall under this plane (internal rotation, external rotation).
An axis is a straight line around which a limb rotates. Movement at a joint takes place in a plane about an axis. There are three axes of rotation that correspond to each of the three planes:
- Sagittal plane: medio-lateral axis
- Frontal plane: anteroposterior axis
- Transverse plane: longitudinal axis
There is a tendency when describing a movement to refer it to the particular plane that it is dominated by. For example, running is often considered to be a movement in the sagittal plane. In reality, all movements involves movements in more than one dimension.
Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward. Refer to Figure 1 as you go through this section.

Watch this video to learn about anatomical motions. What motions involve increasing or decreasing the angle of the foot at the ankle?

Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (see Figure 1 a-d ).
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (see Figure 1 e ).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints, and at multiaxial ball-and-sockets joints (see Figure 1 e ).
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation . Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (see Figure 1 f ). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position , and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (see Figure 2 g ).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (see Figure 2 h ).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (see Figure 2 i ).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially, toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward. (See Figure 2 j .)
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces opening of the mouth (see Figure 2 k ).
Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Superior Rotation and Inferior Rotation
Superior and inferior rotation are movements of the scapula and are defined by the direction of movement of the glenoid cavity. These motions involve rotation of the scapula around a point inferior to the scapular spine and are produced by combinations of muscles acting on the scapula. During superior rotation , the glenoid cavity moves upward as the medial end of the scapular spine moves downward. This is a very important motion that contributes to upper limb abduction. Without superior rotation of the scapula, the greater tubercle of the humerus would hit the acromion of the scapula, thus preventing any abduction of the arm above shoulder height. Superior rotation of the scapula is thus required for full abduction of the upper limb. Superior rotation is also used without arm abduction when carrying a heavy load with your hand or on your shoulder. You can feel this rotation when you pick up a load, such as a heavy book bag and carry it on only one shoulder. To increase its weight-bearing support for the bag, the shoulder lifts as the scapula superiorly rotates. Inferior rotation occurs during limb adduction and involves the downward motion of the glenoid cavity with upward movement of the medial end of the scapular spine.
Opposition and Reposition
Opposition is the thumb movement that brings the tip of the thumb in contact with the tip of a finger. This movement is produced at the first carpometacarpal joint, which is a saddle joint formed between the trapezium carpal bone and the first metacarpal bone. Thumb opposition is produced by a combination of flexion and abduction of the thumb at this joint. Returning the thumb to its anatomical position next to the index finger is called reposition (see Figure 2 l ).
Chapter Review
The variety of movements provided by the different types of synovial joints allows for a large range of body motions and gives you tremendous mobility. These movements allow you to flex or extend your body or limbs, medially rotate and adduct your arms and flex your elbows to hold a heavy object against your chest, raise your arms above your head, rotate or shake your head, and bend to touch the toes (with or without bending your knees).
Each of the different structural types of synovial joints also allow for specific motions. The atlantoaxial pivot joint provides side-to-side rotation of the head, while the proximal radioulnar articulation allows for rotation of the radius during pronation and supination of the forearm. Hinge joints, such as at the knee and elbow, allow only for flexion and extension. Similarly, the hinge joint of the ankle only allows for dorsiflexion and plantar flexion of the foot.
Condyloid and saddle joints are biaxial. These allow for flexion and extension, and abduction and adduction. The sequential combination of flexion, adduction, extension, and abduction produces circumduction. Multiaxial plane joints provide for only small motions, but these can add together over several adjacent joints to produce body movement, such as inversion and eversion of the foot. Similarly, plane joints allow for flexion, extension, and lateral flexion movements of the vertebral column. The multiaxial ball and socket joints allow for flexion-extension, abduction-adduction, and circumduction. In addition, these also allow for medial (internal) and lateral (external) rotation. Ball-and-socket joints have the greatest range of motion of all synovial joints.
Interactive Link Questions
Dorsiflexion of the foot at the ankle decreases the angle of the ankle joint, while plantar flexion increases the angle of the ankle joint.
Answers for Review Questions
Answers for Critical Thinking Questions
- Ball-and-socket joints are multiaxial joints that allow for flexion and extension, abduction and adduction, circumduction, and medial and lateral rotation.
- To cross your arms, you need to use both your shoulder and elbow joints. At the shoulder, the arm would need to flex and medially rotate. At the elbow, the forearm would need to be flexed.
Biomechanics of Human Movement Copyright © August 22, 2016 by OpenStax is licensed under a Creative Commons Attribution 4.0 International License , except where otherwise noted.
Share This Book
Anatomical Terms of Movement
Written by Oliver Jones
Last updated May 30, 2020 • 27 Revisions •
Anatomical terms of movement are used to describe the actions of muscles upon the skeleton. Muscles contract to produce movement at joints, and the subsequent movements can be precisely described using this terminology.
The terms used assume that the body begins in the anatomical position . Most movements have an opposite movement – also known as an antagonistic movement. We have described the terms in antagonistic pairs for ease of understanding.
Premium Feature
Flexion and extension.
Flexion and extension are movements that occur in the sagittal plane. They refer to increasing and decreasing the angle between two body parts:
Flexion refers to a movement that decreases the angle between two body parts. Flexion at the elbow is decreasing the angle between the ulna and the humerus. When the knee flexes, the ankle moves closer to the buttock, and the angle between the femur and tibia gets smaller.
Extension refers to a movement that increases the angle between two body parts. Extension at the elbow is increasing the angle between the ulna and the humerus. Extension of the knee straightens the lower limb.
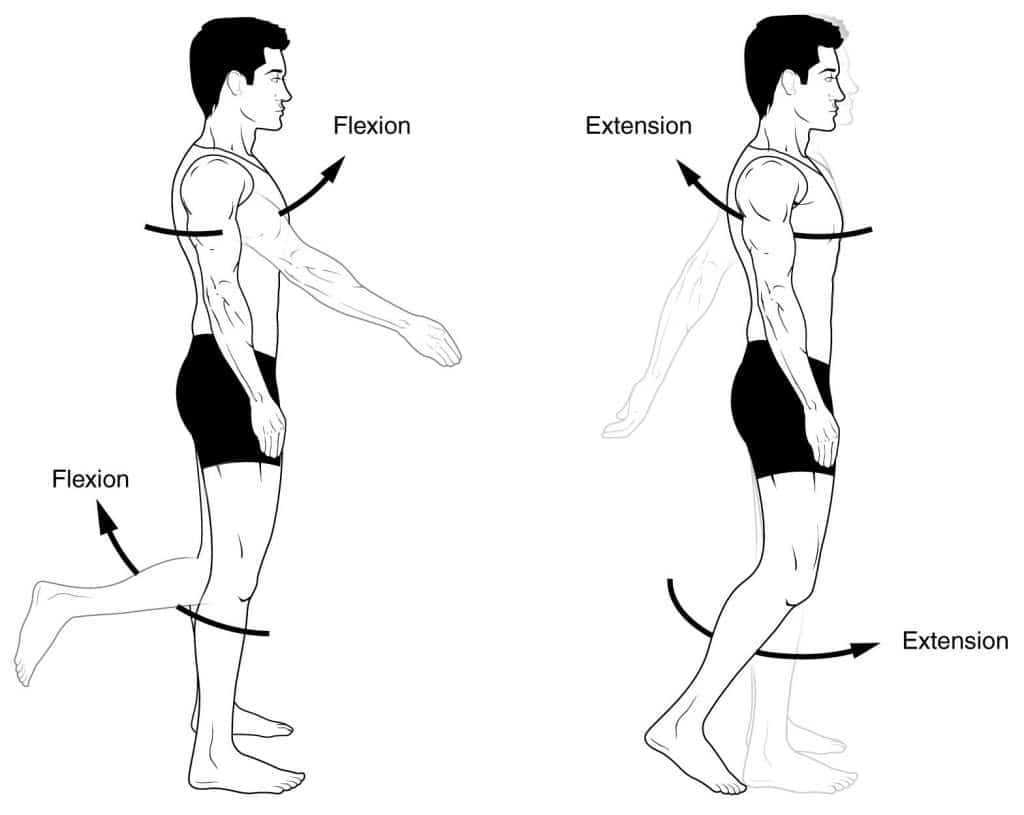
Fig 1 Flexion and extension.
Abduction and Adduction
Abduction and adduction are two terms that are used to describe movements towards or away from the midline of the body.
Abduction is a movement away from the midline – just as abducting someone is to take them away. For example, abduction of the shoulder raises the arms out to the sides of the body.
Adduction is a movement towards the midline. Adduction of the hip squeezes the legs together.
In fingers and toes, the midline used is not the midline of the body, but of the hand and foot respectively. Therefore, abducting the fingers spreads them out.
Medial and Lateral Rotation
Medial and lateral rotation describe movement of the limbs around their long axis:
Medial rotation is a rotational movement towards the midline. It is sometimes referred to as internal rotation. To understand this, we have two scenarios to imagine. Firstly, with a straight leg, rotate it to point the toes inward. This is medial rotation of the hip. Secondly, imagine you are carrying a tea tray in front of you, with elbow at 90 degrees. Now rotate the arm, bringing your hand towards your opposite hip (elbow still at 90 degrees). This is internal rotation of the shoulder.
Lateral rotation is a rotating movement away from the midline. This is in the opposite direction to the movements described above.
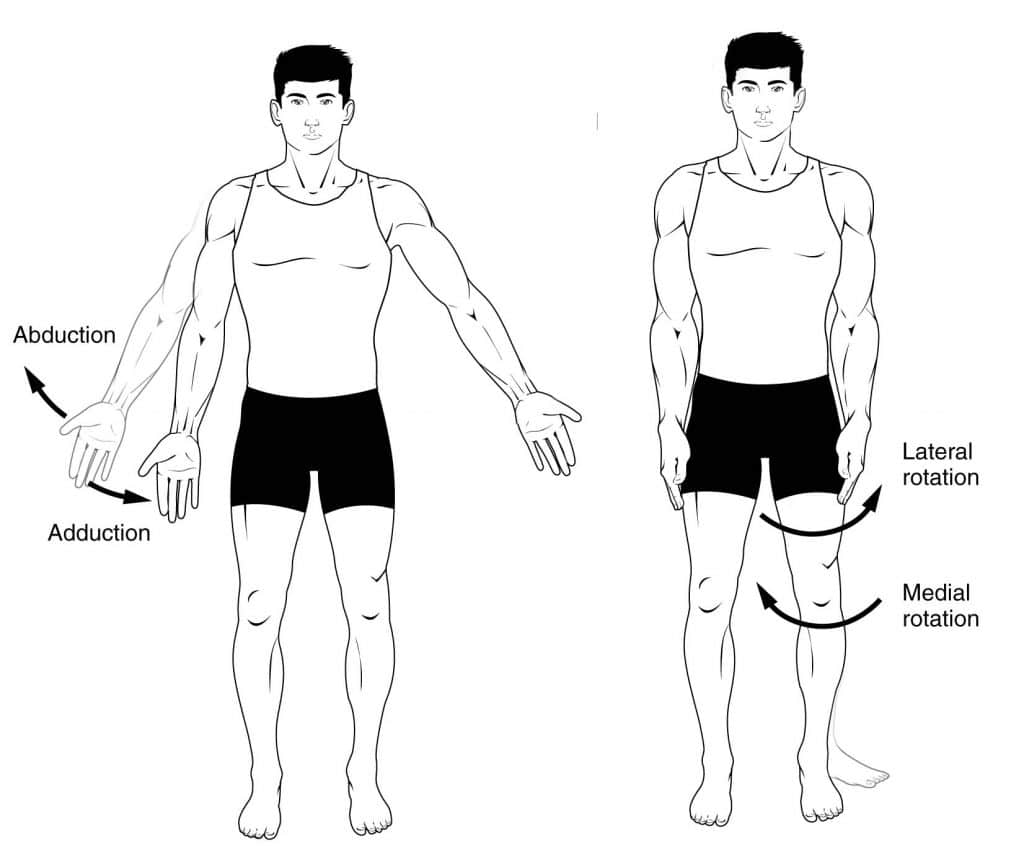
Fig 2 Adduction, abduction and rotation.
Elevation and Depression
Elevation refers to movement in a superior direction (e.g. shoulder shrug), depression refers to movement in an inferior direction.
Pronation and Supination
This is easily confused with medial and lateral rotation, but the difference is subtle. With your hand resting on a table in front of you, and keeping your shoulder and elbow still, turn your hand onto its back, palm up. This is the supine position, and so this movement is supination .
Again, keeping the elbow and shoulder still, flip your hand onto its front, palm down. This is the prone position, and so this movement is named pronation .
These terms also apply to the whole body – when lying flat on the back, the body is supine. When lying flat on the front, the body is prone.
Dorsiflexion and Plantarflexion
Dorsiflexion and plantarflexion are terms used to describe movements at the ankle. They refer to the two surfaces of the foot; the dorsum (superior surface) and the plantar surface (the sole).
Dorsiflexion refers to flexion at the ankle, so that the foot points more superiorly. Dorsiflexion of the hand is a confusing term, and so is rarely used. The dorsum of the hand is the posterior surface, and so movement in that direction is extension . Therefore we can say that dorsiflexion of the wrist is the same as extension.
Plantarflexion refers extension at the ankle, so that the foot points inferiorly. Similarly there is a term for the hand, which is palmarflexion.
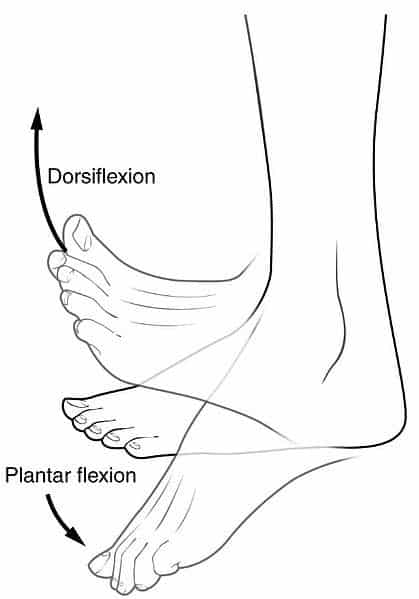
Fig 3 Dorsiflexion and plantar flexion
Inversion and Eversion
Inversion and eversion are movements which occur at the ankle joint, referring to the rotation of the foot around its long axis.
Inversion involves the movement of the sole towards the median plane – so that the sole faces in a medial direction.
Eversion involves the movement of the sole away from the median plane – so that the sole faces in a lateral direction.
Opposition and Reposition
A pair of movements that are limited to humans and some great apes, these terms apply to the additional movements that the hand and thumb can perform in these species.
Opposition brings the thumb and little finger together.
Reposition is a movement that moves the thumb and the little finger away from each other, effectively reversing opposition.
Circumduction
Circumduction can be defined as a conical movement of a limb extending from the joint at which the movement is controlled.
It is sometimes talked about as a circular motion, but is more accurately conical due to the ‘cone’ formed by the moving limb.
Protraction and Retraction
Protraction describes the anterolateral movement of the scapula on the thoracic wall that allows the shoulder to move anteriorly. In practice, this is the movement of ‘reaching out’ to something.
Retraction refers to the posteromedial movement of the scapula on the thoracic wall, which causes the shoulder region to move posteriorly i.e. picking something up.
Do you think you’re ready? Take the quiz below
Question 1 of 3
Recommended Reading
Forgot password.
Please enter your username or email address below. You will receive a link to create a new password via emai and please check that the email hasn't been delivered into your spam folder.
We use cookies to improve your experience on our site and to show you relevant advertising. To find out more, read our privacy policy .
Privacy Overview
Report question, rate this article.

TMJ Movements
Normal movements of the jaw during function, such as chewing, are known as excursions. There are two lateral excursions ( left and right ) and the forward excursion, known as protrusion, the reversal of which is retrusion.
When the jaw is moved into protrusion, the lower incisors or front teeth are moved so that they first come edge to edge with the upper incisors, and then move past them, producing a temporary underbite. This is accomplished by sliding of the condyle down the articular eminance ( in the upper portion of the TMJ ) without any more than the slightest amount of rotation taking place ( in the lower portion of the TMJ ), other than that necessary to allow the lower incisors to come in front of the upper incisors without running into them.
During chewing, the jaw moves in a specific manner as delineated by the two TMJs. The side of the mandible that moves sideways is referred to as either the working or rotating side, while the other side is referred to as either the balancing or orbiting side. The latter terms, although a bit outdated, are actually more precise, as they define the sides by the movements of the respective condyles. When the jaw is moved into a lateral excursion, the working side condyle ( the condyle on the side of the jaw that moves outwards ) only performs rotation ( in the horizontal plane ), while the balancing side condyle performs translation. During actual functional chewing, when the teeth are not only moved side to side, but also up and down when biting of the teeth is incorporated as well, rotation ( in a vertical plane ) also plays a part in both condyles.
The jaw is moved primary by four muscles: the masseter, medial pterygoid, lateral pterygoid and the temporalis. These four muscles work in different groups to move the mandible in different directions. Contraction of the lateral pterygoid acts to pull the disc and condyle forward; thus, the action of this muscle serves to open the mouth. The other three muscles close the mouth; the masseter and the medial pterygoid by pulling up the angle of the mandible and the temporalis by pulling up on the coronoid process.
When the mouth opens, two distinct motions occur at the joint. The first motion is ROTATION around a horizontal axis through the condylar heads. The second motion is TRANSLATION. The condyle and meniscus move together interiorly beneath the articular eminence.
In the closed mouth position, the thick posterior band of the meniscus lies immediately above the condyle. As the condyle translates forward, the thinner intermediate zone of the meniscus becomes the articulating surface between the condyle and the articular eminence. When the mouth is fully open, the condyle may lie beneath the anterior band of the meniscus.
Musculoskeletal Key
Fastest musculoskeletal insight engine.
- MANUAL THERAPIST
- MUSCULOSKELETAL MEDICINE
- PHYSICAL MEDICINE & REHABILITATION
- RHEUMATOLOGY
- SPORT MEDICINE
- Gold Membership
The Temporomandibular Joint
CHAPTER 26 The Temporomandibular Joint CHAPTER OBJECTIVES At the completion of this chapter, the reader will be able to: Describe the anatomy of the temporomandibular joint (TMJ), including the bones, ligaments, muscles, and blood and nerve supply. Describe the biomechanics of the TMJ, including the movements, normal and abnormal joint barriers, kinesiology, and reactions to various stresses. Summarize the various causes of temporomandibular dysfunction (TMD). Describe the close association between the TMJ, the middle ear, and the cervical spine. Perform a comprehensive examination of the temporomandibular musculoskeletal system, including palpation of the articular and soft-tissue structures, specific passive mobility, and passive articular mobility tests, and stability tests. Evaluate the total examination data to establish a diagnosis. Recognize the manifestations of abnormal TMJ function and develop strategies to correct these abnormalities. Apply active and passive mobilization techniques to the TMJ, using the correct grade, direction, and duration. Describe and demonstrate intervention strategies and techniques based on clinical findings and established goals. Evaluate the intervention effectiveness in order to progress or modify an intervention. Plan an effective home program and instruct the patient in this program. OVERVIEW Approximately 50–75% of the general population has experienced unilateral temporomandibular joint dysfunction (TMD) on a minimum of one occasion and that at least 33% have reported a minimum of one continuing persistent symptom. 1 , 2 TMD is a collective term used to describe a number of related disorders affecting the stomatognathic system and its related structures, all of which may have common symptoms. The term TMJ dysfunction as an overall descriptor of stomatognathic system dysfunction has been discontinued because it implies structural problems when none may exist, and does not include the many other factors that may be involved. 3 Housed within the skull are the components of the stomatognathic system, which includes the TMJ, the masticatory systems, and the related organs and tissues such as the inner ear and salivary glands. 4 An interrelationship exists between the stomatognathic system and the head and neck due to their proximity and shared embryological development. An understanding of this relationship is vital to understand the reasons for the myriad of symptoms that this region can exhibit. The embryologic structures from which the head, the face, and the neck originate are segmentally organized during development with the appearance and modification of six paired branchial or pharyngeal arches. 4 These branchial arches contain the cranial nuclei of the trigeminal nerve (ophthalmic; maxillary and mandibular), the facial, the glossopharyngeal, and the laryngeal branch of the vagus nerve as well as the hypoglossal nerve. The first of these arches, the mandibular arch, consists of a large anterior (ventral) part (the mandibular process of Meckel’s cartilage) and a small posterior (dorsal) (maxillary) process. As development progresses, both processes disappear except for two small portions at the posterior (dorsal) ends, which persist. The first brachial arch forms the mandible; the rudiments of the inner ear bones, the malleus, and incus; the anterior malleolar and sphenomandibular ligaments of the TMJ; the tensor tympani and the tensor veli palatini of the inner ear; the mylohyoid and the anterior belly of the digastric muscle; and the trigeminal mandibular nerve. The second pharyngeal arch (the hyoid arch) consists of Reichert’s cartilage. This arch is involved in the formation of the superior component of the hyoid bone and the lesser cornu bone; the stapes muscle; the temporal styloid process; the stylohyoid ligament; the stapedius muscle; the stylohyoid muscle; the posterior belly of the digastric muscle; the muscles of facial expression and mastication; the platysma muscle; and the glossopharyngeal nerve. The third pharyngeal arch is involved in the formation of the greater cornu of the hyoid and its body, the stylopharyngeal muscle, and the sensory apparatus of the posterior one-third of the tongue. The fourth pharyngeal arch combines with the sixth arch to form the thyroid, cricoid, and arytenoid cartilages of the larynx. The muscles derived from this arch are the pharyngeal constrictors (the cricothyroid) and the intrinsic muscles of the larynx. The pharyngeal constrictors are innervated by the superior laryngeal branch of the vagus nerve. The intrinsic muscles of the larynx are innervated by the recurrent laryngeal branch of the vagus nerve. In primitive creatures, and the human fetus, vibrations through the jaw are used as a basis for hearing. At around 8½ weeks, the small bones of the inner ear (the malleus, incus, and stapes) can be seen as distinct entities. The development of the malleus bone and the tensor tympani are intimately related to that of the lateral pterygoid muscle. Due to this embryological relationship, it is theorized that a spasm of the lateral pterygoid muscle can increase the tension within the tensor tympani (similar to that of a drum skin) 4 resulting in increased sensitivity to pitch and vibration. Theoretically, this increased tension could produce sensorineural tinnitus, or ringing in the ears, 4 a common associated symptom of a TMD, and an injury to the craniovertebral region. The diagnosis of TMD, like that of whiplash syndrome, remains controversial. 5 This is due in part to a paucity of studies regarding the incidence, course, management, and prognosis of claimed TMDs. 6 , 7 However, reports of TMD appear to be quite common. Although 50–75% of the general population has at least one sign of a TMD, only around one in four people with signs is actually aware of, or reports, any symptoms, 8 , 9 and only about 5% of people with one or more signs of a TMD will actually seek an intervention. 9–11 TMD tends to affect women more often than men, 12 specifically women over the age of 55. 13 After a technology assessment conference in 1996 about managing TMD, the National Institutes of Health (NIH) concluded that the natural history and etiology of TMD are not well understood and that most TMD symptoms are self-limiting, can recur, and may fluctuate over time. 14 The most common TMD by far, comprising 90–95% of all TMD cases, is a condition with multiple musculoskeletal facial pain complaints and a variety of jaw impairments, without an identified structural cause. 15 Due to the complex interplay between the sympathetic and trigeminal nervous systems and an increased understanding of the centralization of pain, TMD is best approached as a cluster of related disorders in the stomatognathic system that have many causes and common symptoms. 16 There are likely three etiologic factors of TMD: (1) predisposing factors, (2) precipitating or triggering factors, and (3) perpetuating or sustaining factors 17 : Predisposing factors include the structural, neurologic, hormonal, and metabolic features of an individual. Precipitating factors generally fall into the following four categories: (1) overt, extrinsic trauma to the head, the neck, or the jaw; (2) repeated low-grade extrinsic trauma, such as nail biting and chewing gum; (3) repeated low-grade intrinsic trauma such as teeth clenching or bruxism (grinding teeth); and (4) stress that passes a certain threshold, which is individual for each patient. Perpetuating or contributing factors are those that aid in the continuation of symptoms. These can include systemic disease and cervical pathology. Thus, the clinical course of TMD does not reflect a progressive disease but rather a complex disorder that is molded by many interacting factors, such as stress, anxiety, and depression, which serve to maintain the disease. 16 Headaches, orofacial pain, earache, and neck pain are common complaints. A diagnosis of TMD must, therefore, include an examination of all of the following: Jaw muscles Bone and cartilage joint structures Facial structures Soft-tissue joint structures, including the articular disk and synovium Jaw and joint function Cervical and upper thoracic spine function Posture and dysfunction Systemic disease Psychosocial issues Given the number of potential causes of jaw and face pain, a diagnosis of TMD can rarely be ascribed solely to the TMJ. Examples of appropriate diagnoses for TMD are more likely to include rheumatoid arthritis with synovitis, arthralgia, condylar degenerative disease, and open bite deformity; chronic pain with a behavioral disorder; myofascial pain and impairment; and internal disk derangement, with displacement and reduction. CLINICAL PEARL Most of those who seek medical intervention for TMDs are female. The reason for the higher prevalence of TMD in women, and the overrepresentation of females at orofacial pain clinics remains obscure. One explanation could be that women more readily seek treatment for illness than do men. 18
Nonsurgical interventions such as counseling, physical therapy, pharmacotherapy, and occlusal splint therapy continue to be the most effective way of managing more than 80% of patients with TMD. 16 Although dentists are the primary professionals involved in the examination and intervention of TMD, physical therapists can play an important role in assisting the dentist in restoring function to the stomatognathic system. However, the procedures in physical therapy intervention are not well described in the literature in this area. ANATOMY The TMJ ( Fig. 26-1 ) is a synovial, compound, modified ovoid bicondylar joint, which is formed between the articular eminence of the temporal bone, the intra-articular disk, and the head of the mandible. FIGURE 26-1 The temporomandibular joint. (Reproduced, with permission, from Chapter 21 . Infratemporal Fossa. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) The TMJ is unique in that, even though the joint is synovial, the articulating surfaces of the bones are covered not by hyaline cartilage but by fibrocartilage. 19 , 20 Fibrocartilage has the same general properties found in hyaline cartilage but tends to be less distensible, owing to a greater proportion of dense collagen fibers (see Chapter 1 ). The development of fibrocartilage over the load-bearing surface of the TMJ indicates that the joint is designed to withstand large and repeated stresses and that this area of the joint surface has a greater capacity to repair itself than would hyaline cartilage. 21 The area of load bearing is affected by the congruity of the contacting tooth surfaces (occlusion), head position, and the coordination of muscle function. The fibrocartilage is at its thinnest at the roof of the fossa, but load bearing here occurs only in the presence of dysfunction. 22 The mandible works like a class-three lever (see Chapter 1 ), with its joint as the fulcrum. Although there is no agreement among the experts concerning force transmission through the joint, there does appear to be agreement that postural impairments of the cervical and upper thoracic spine can produce both pain and impairment of the TMJ. 8 Bony Anatomy
A number of bony components make up the masticatory system: the maxilla and the mandible, which support the teeth, and the temporal bone, which supports the mandible at its articulation with the skull. The sphenoid bone and the hyoid bone also could be included, because they provide important anatomic and functional links to the TMJ. Maxilla
The borders of the maxillae extend superiorly to form the floor of the nasal cavity as well as the floor of each orbit ( Fig. 26-1 ). Inferiorly, the maxillary bones form the palate and the alveolar ridges, which support the teeth. The maxillae and mandible each contains 16 permanent teeth. The structure of each tooth reflects its function in mastication. Sphenoid Bone
The greater wings of the sphenoid bone form the boundaries of the anterior part of the middle cranial fossa. From these greater wings, the pterygoid laminae serve as the attachments for the medial and lateral pterygoid muscles. Hyoid Bone
The U-shaped hyoid bone ( Fig. 26-2 ), also known as the skeleton of the tongue, serves as the attachment for the infrahyoid muscles and for some of the extrinsic tongue muscles. The hyoid bone is involved with the mandible to provide reciprocal stabilization during swallowing and chewing. Theoretically, due to its muscle attachments, the position of the hyoid bone can be affected by cervical and shoulder positions, as occurs during forward head posture, which changes the length–tension relationships. FIGURE 26-2 The hyoid bone and related muscles. (Reproduced, with permission, from Chapter 25 . Overview of the Neck. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy . New York, NY: McGraw-Hill; 2011.) Mandible
The mandible, or jaw ( Fig. 26-1 ), which supports the lower teeth, is the largest and the strongest bone in the face. It is suspended below the maxillae by muscles and ligaments that provide it with both mobility and stability. The medial surface of the mandible serves as the attachment for the medial pterygoid and the digastric muscles. The platysma, mentalis, and buccinator gain attachment on its lateral aspect. Two broad, vertical rami extend upward from the mandible: the condyle and the coronoid process. The anterior of the two processes, the coronoid, serves as the attachment for the temporalis and masseter muscles. 23 The condyle process articulates with the temporal bone. The bony surfaces of the condyle and the articular portion of the temporal bone are made of dense cortical bone. The articulating surface of the condyle is flattened from front to back with its medial–lateral length twice as long as its anterior–posterior length. The condyles are generally convex, possessing short bony projections known as medial and lateral poles. 24 Temporal Bone
The mandibular fossa of the temporal bone is divided into two surfaces: articular and nonarticular. 24 The articulating surface of the temporal bone is made up of a concave mandibular, or glenoid, fossa and a convex bony prominence called the articular eminence. 25 The articular tubercle, situated anterior to the glenoid fossa, serves as an attachment for the temporomandibular (or lateral) ligament. 23 The nonarticular surface of the fossa consists of a very thin layer of bone and fibrocartilage that occupies much of the superior and posterior walls of the fossa. 24 Fibrocartilaginous Disk
Located between the articulating surface of the temporal bone and the mandibular condyle is a fibrocartilaginous disk (sometimes inappropriately referred to as “meniscus”) ( Fig. 26-3 ). The biconcave shape of the disk is determined by the shape of the condyle and the articulating fossa. 26 Rees 20 has described the fibrocartilaginous disk as having three clearly defined transverse, ellipsoidal zones that are divided into three regions—posterior band, intermediate zone, and anterior band—of which the intermediate zone makes contact with the articular surface of the condyle. FIGURE 26-3 The TMJ disk and the pterygoid. (Reproduced, with permission, from Chapter 21 . Infratemporal Fossa. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy . New York, NY: McGraw-Hill; 2011.) Both the disk and the lateral pterygoid muscle develop from the first branchial arch, and there is very little differentiation among the muscle, the disk, and the joint capsule. 27 , 28 The fibrocartilaginous disk is tethered by a number of structures: Medial and lateral collateral diskal ligaments firmly attach the fibrocartilaginous disk to the medial and lateral poles of the condyle, permitting anterior and posterior rotation of the disk on the condyle during mouth opening and closing. 29 , 30 Posteriorly, the disk is attached by fibroelastic tissue to the posterior mandibular fossa and the back of the mandibular condyle. 29 , 30 Anteriorly, the disk is attached to the upper part of the tendon of the lateral pterygoid muscle ( Fig. 26-3 ). 29 , 30 The disk usually is located on top of the condyle in the 12 o’clock to 1 o’clock position on the mandibular head when the jaw is closed. 31 Since the only firm attachment of the disk to the condyle occurs medially and laterally, the disk can move somewhat independently of the condyle. 32 The disk effectively divides the TMJ into a lower and an upper joint cavity (see Fig. 26-3 ): Lower compartment. This compartment, bordered by the mandibular condyle and the inferior surface of the articular disk, is where, under normal conditions, the osteokinematic spin (rotation) of the condyle occurs. 8 Upper compartment. This compartment, bordered by the mandibular fossa and the superior surface of the articular disk, primarily allows only translation of the disk and condyle along the fossa, and onto the articular eminence. 8 Blood vessels and nerves are found only in the thickened periphery of this disk, especially its posterior attachment; its middle articular portion is avascular and aneural. 33 Supporting Structures
The supporting structures of the TMJ consist of periarticular connective tissue (ligament, tendon, capsule, and fascia). As its name implies, the periarticular connective tissue serves to keep the joints together and to limit the ranges of motion at the joint. For example, the ligaments of the TMJ protect and support the joint structures and act as passive restraints to joint movement. The synovial cavities are surrounded by loose connective tissue rather than by ligaments. The intercapsular structures are located posteriorly to the condyle. Anterior to the joint are the muscles of the medial and lateral pterygoid (see next section). There are no well-defined anterior or posterior ligaments between the mandibular condyle and the temporal bone. However, two strong ligaments help to provide joint stability: Joint capsule or capsular ligament. This structure, which surrounds the entire joint, is thought to provide proprioceptive feedback regarding the joint position and movement. 34 , 35 Temporomandibular (or lateral) ligament. The capsule of the TMJ is reinforced laterally by an outer oblique portion and an inner horizontal portion of the temporomandibular ligament, which function as a suspensory mechanism for the mandible during moderate opening movements. The ligament also functions to resist rotation and posterior displacement of the mandible. Two other ligaments assist with joint stability: Stylomandibular ligament. The stylomandibular ligament is a specialized band that splits away from the superficial lamina of the deep cervical fascia to run deep to both pterygoid muscles. 25 This ligament becomes taut and acts as a guiding mechanism for the mandible, keeping the condyle, disk, and temporal bone firmly opposed. Sphenomandibular ligament. The sphenomandibular ligament is a thin band that runs from the spine of the sphenoid bone to a small bony prominence on the medial surface of the ramus of the mandible, called the lingula. This ligament acts to check the angle of the mandible from sliding as far forward as the condyles during the translatory cycle and serves as a suspensory ligament of the mandible during wide opening. 25 It is this ligament that hurts with any prolonged jaw opening, such as that which occurs at the dentist. CLINICAL PEARL Pinto’s ligament 36 is a vestige of Meckel’s cartilage, an embryological tissue. It arises from the neck of the malleus of the inner ear and runs in a medial-superior direction to insert into the posterior aspect of the TMJ capsule and disk. While the role of this ligament in mandibular mechanics is thought to be negligible, its relationship to the middle ear and the TMJ could be a basis for the middle ear symptoms, which are often present with TMD. Stack and Funt 37 postulated that auditory symptoms of fullness and pressure in the middle ear might be present as a result of direct transmission of TMJ capsular tension to the ossicles of the middle ear through this ligament. Muscles
The muscles of mastication are the key muscles when discussing TMD. Three of these muscles, the masseter, the medial pterygoid, and the temporalis ( Fig. 26-4 ), function to raise the mandible during mouth closing. The lateral pterygoid and digastric muscles work together to depress the mandible during mouth opening. FIGURE 26-4 Lateral view of TMJ. (Reproduced, with permission, from Chapter 21 . Infratemporal Fossa. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy. New York, NY: McGraw-Hill; 2011.) Although these muscles work most efficiently in groups, an understanding of the specific anatomy and action(s) of the individual muscles is necessary for an appreciation of their coordinated function during masticatory activity ( Tables 26-1 and 26-2 ). TABLE 26-1 Muscles of the Temporomandibular Joint Muscle Proximal Distal Innervation Medial pterygoid Medial surface of lateral pterygoid plate and tuberosity of maxilla Medial surface of mandible close to angle Mandibular division of trigeminal nerve Lateral pterygoid Greater wing of sphenoid and lateral pterygoid plate Neck of mandible and articular cartilage Mandibular division of trigeminal nerve Temporalis Temporal cranial fossa By way of a tendon into medial surface, apex, and anterior and posterior borders of mandibular ramus Anterior and posterior deep temporal nerves, which branch from anterior division of mandibular branch of trigeminal nerve Masseter Superficial portion: from anterior two-thirds of lower border of zygomatic arch; deep portion from medial surface of zygomatic arch Lateral surfaces of coronoid process of mandible, upper half of ramus, and angle of mandible Masseteric nerve from anterior trunk of mandibular division of trigeminal nerve Mylohyoid Medial surface of mandible Body of hyoid bone Mylohyoid branch of trigeminal nerve and mandibular division Geniohyoid Mental spine of mandible Body of hyoid bone Anterior (ventral) ramus of C1 via hypoglossal nerve Stylohyoid Styloid process of temporal bone Body of hyoid bone Facial nerve Anterior and posterior digastric Internal surface of mandible and mastoid process of temporal bone By intermediate tendon to hyoid bone Anterior: mandibular division of trigeminal nerve; posterior: facial nerve Sternohyoid Manubrium and medial end of clavicle Body of hyoid bone Ansa cervicalis Omohyoid Superior angle of scapula Inferior body of hyoid bone Ansa cervicalis Sternothyroid Posterior surface of manubrium Thyroid cartilage Ansa cervicalis Thyrohyoid Thyroid cartilage Inferior body and greater horn of hyoid bone C1 via hypoglossal nerve TABLE 26-2 Actions of the Temporomandibular Joint Muscles Action Muscles Acting Opening of mouth Lateral pterygoid Mylohyoid Geniohyoid Digastric Closing of mouth Masseter Temporalis Medial pterygoid Protrusion of mandible Lateral pterygoid Medial pterygoid Masseter Mylohyoid Geniohyoid Digastric Stylohyoid Temporalis (anterior fibers) Retraction of mandible Temporalis (posterior fibers) Masseter Digastric Stylohyoid Mylohyoid Geniohyoid Lateral deviation of mandible Lateral pterygoid (ipsilateral muscle) Medial pterygoid (contralateral muscle) Temporalis Masseter Temporalis
The temporalis muscle ( Fig. 26-4 ) has its origin from the floor of the temporal fossa and the temporal fascia. The muscle travels inferiorly and anteriorly to insert on the anterior border of the coronoid process and the anterior border of the ramus of the mandible. The temporalis muscle is innervated by a branch of the mandibular division of the trigeminal nerve. In addition to assisting with mouth closing and side-to-side grinding of the teeth, the temporalis muscle provides a good deal of stability to the joint. The Masseter
The masseter ( Fig. 26-4 ) is a two-layered quadrilateral-shaped muscle. The superficial portion arises from the anterior two-thirds of the lower border of the zygomatic arch. The deep portion arises from the medial surface of the zygomatic arch. Both sets of fibers blend anteriorly and form a raphe with the medial pterygoid. 25 The masseter inserts on the lateral surface of the coronoid process of the mandible, the upper half of the ramus and angle of the mandible. The masseter muscle is innervated by a branch of the mandibular division of the trigeminal nerve. The major function of the masseter is to elevate the mandible, thereby occluding the teeth during mastication. The Medial Pterygoid
The medial pterygoid muscle is a thick quadrilateral muscle, with a deep origin situated on the medial aspect of the mandibular ramus ( Fig. 26-4 ). The muscle travels posteriorly to insert on the inferior and posterior aspects of the medial subsurface of the ramus and angle of the mandible. The medial pterygoid muscle is innervated by a branch of the mandibular division of the trigeminal nerve. Working bilaterally, and in association with the masseter and temporalis muscles, the medial pterygoids assist in mouth closing. Individually, the medial pterygoid muscle is capable of deviating the mandible toward the opposite side. The medial pterygoid muscle also assists the lateral pterygoid and anterior fibers of the temporalis muscle to produce protrusion of the mandible. The Lateral Pterygoid
Two divisions of the lateral pterygoid muscles are recognized, each of which is functionally and anatomically separate ( Figs. 26-3 and 26-4 ). The superior head arises from the infratemporal surface of the greater wing of the sphenoid. The inferior head arises from the lateral surface of the lateral pterygoid plate. Despite several investigations, 38–40 no consensus has been reached regarding the insertion of the lateral pterygoid muscle. However, the most commonly described insertion is at the anterior aspect of the neck of the mandibular condyle and capsule of the TMJ. The lateral pterygoid muscle is innervated by a branch of the mandibular division of the trigeminal nerve. The superior head of the lateral pterygoid is involved mainly with chewing and functions to rotate the disk anteriorly on the condyle during the closing movement. 41 , 42 It has also been suggested that in normal function of the craniomandibular complex, the superior lateral pterygoid plays an important role in stabilizing and controlling the movements of the disk. 43 The inferior head of the lateral pterygoid muscle exerts an anterior, lateral, and inferior pull on the mandible, thereby opening the jaw, protruding the mandible, and deviating the mandible to the opposite side. Infrahyoid or “Strap” Muscles
The infrahyoid muscles comprise the sternohyoid, omohyoid, sternothyroid, and thyrohyoid muscles ( Fig. 26-5 ). FIGURE 26-5 The infrahyoid muscles. (Reproduced, with permission, from Chapter 25 . Overview of the Neck. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy . New York, NY: McGraw-Hill; 2011.) Sternohyoid The sternohyoid muscle is a strap-like muscle that functions to depress the hyoid and assist in speech and mastication. Omohyoid The omohyoid muscle, situated lateral to the sternohyoid, consists of two bellies and functions to depress the hyoid. In addition, the muscle has been speculated to tense the inferior aspect of the deep cervical fascia in prolonged inspiratory efforts, thereby releasing tension on the apices of the lungs and on the internal jugular vein, which are attached to this fascial layer. 25 Sternothyroid and Thyrohyoid The sternothyroid and thyrohyoid muscles (see Fig. 26-5 ) are located deep to the sternohyoid muscle. The sternothyroid muscle is involved in drawing the larynx downward, whereas the thyrohyoid depresses the hyoid and elevates the larynx. These infrahyoid muscles are innervated by fibers from the upper cervical nerves. The nerves to the lower part of these muscles are given off from a loop, the ansa cervicalis (cervical loop) (see Chapter 3 ). Suprahyoid Muscles
The suprahyoid muscles ( Fig. 26-2 ), working with the infrahyoid muscles, play a major role in coordinating mandibular function, by providing a firm base on which the tongue and mandible can be moved. Geniohyoid The geniohyoid muscle is a narrow muscle situated under the mylohyoid muscle. The muscle functions to elevate the hyoid bone. Digastric As its name suggests, the digastric muscle consists of two bellies. The posterior belly arises from the mastoid notch of the temporal bone while the anterior belly arises from the digastric fossa of the mandible. The posterior belly is innervated by a branch of the facial nerve. The anterior belly is innervated by the inferior alveolar branch of the trigeminal nerve. The two bellies of the digastric muscle are joined by a rounded tendon that attaches to the body and greater cornu of the hyoid bone through a fibrous loop or sling. 25 Bilaterally, the two bellies of the digastric muscle assist in forced mouth opening by stabilizing the hyoid. The posterior bellies are especially active during coughing and swallowing. 25 CLINICAL PEARL The muscles of the TMJ, working in combinations, are involved as follows: Mouth opening—bilateral action of the lateral pterygoid and digastric muscles. Mouth closing—bilateral action of the temporalis, masseter, and medial pterygoid muscles. Lateral deviation—action of the ipsilateral masseter, and contralateral medial and lateral pterygoid muscles. Protrusion—bilateral action of the lateral pterygoid, medial pterygoid, and anterior fibers of the temporalis muscles. Retrusion—bilateral action of the posterior fibers of the temporalis muscle, the digastric, stylohyoid, geniohyoid, and mylohyoid muscles. Mylohyoid This flat, triangular muscle is functionally a muscle of the tongue, stabilizing or elevating the tongue while swallowing and elevating the floor of the mouth in the first stage of deglutition. 25 Stylohyoid The stylohyoid muscle elevates the hyoid and base of the tongue and has an undetermined role in speech, mastication, and swallowing. Nerve Supply
The TMJ is primarily supplied by three nerves that are part of the mandibular division of the fifth cranial (trigeminal) nerve ( Fig. 26-6 ) ( Box 26-1 ). Portions of the middle ear ossicles, middle ear musculature, and muscles of mastication all originate from the first branchial arch and are innervated by this nerve. Therefore, in a patient with altered bite mechanics, spasm of the muscles of mastication caused by a displaced condyle may cause neuromuscular dysfunction of all the muscles innervated by the trigeminal nerve, including the tensor palatini. 44 FIGURE 26-6 The trigeminal nerve. (Reproduced, with permission, from Chapter 17 . Cranial Nerves. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy . New York, NY: McGraw-Hill; 2011.) Box 26-1 Characteristics of the Trigeminal Nerve Motor Nucleus The anterolateral upper pons. Sensory Nucleus There are two nuclei: (1) the chief sensory nucleus in the posterior (dorsal)-lateral pons and (2) the mesencephalic nucleus, which extends from the chief sensory nucleus upward through the pons to the midbrain. Spinal Nucleus The spinal tract consists of small- and medium-sized myelinated nerve fibers and runs caudally to reach the upper cervical segments of the spinal cord. The lowest nerve fibers in the tract mix with the spinal fibers in the tract of Lissauer. Nerves Mandibular Ophthalmic Maxillary Termination Muscles of mastication, both pterygoids, tensor veli palatini, tensor tympani, mylohyoid, and anterior belly of digastric. Skin of vertex, temporal area, forehead, and face; mucosa of sinuses, nose, pharynx, anterior two-thirds of tongue, and oral cavity. Lacrimal, parotid, and lingual glands; dura of anterior and middle cranial fossae. External aspect of tympanic membrane and external auditory meatus, TMJ, and teeth. Dilator pupillae and probably proprioceptors of extraocular muscles. Sensation from upper three or four cervical levels.
There is considerable clinical interest in the interactions between the cervical and craniofacial regions. This interest stems from a number of reports concerning patients who have pain in the cervical and craniofacial areas simultaneously. 32 , 45–48 In the suboccipital region, a series of dense neural connections, called the trigeminocervical complex, exists among trigeminal, facial, glossopharyngeal, and vagus nerves, with those of the upper C1–4 cervical spinal nerves ( Fig. 26-7 ). 17 Postural abnormalities resulting from various acute or chronic etiologies that produce suboccipital compression may, therefore, be responsible for craniofacial pain anywhere in the head, in addition to symptoms of dizziness or nystagmus. 7 , 17 , 49 FIGURE 26-7 Neurology of the TMJ. (Reproduced, with permission, from Chapter 21 . Infratemporal Fossa. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy . New York, NY: McGraw-Hill; 2011.) TMJ-related headaches usually include pain near the TMJ and ear, ear fullness, temporal headaches, and facial pain. 50 The dizziness associated with TMD tends to be of the nonvertiginous variety, with the patient complaining of unsteadiness, giddiness, or lightheadedness. 51 Although the exact mechanism is unclear, postural influences, alteration in the position of the jaw by the malocclusion, and the subsequent mismatching between the cervical muscles might be the cause. 51 BIOMECHANICS The movements that occur at the TMJ are extremely complex. The TMJ has three degrees of freedom, with each of the degrees of freedom being associated with a separate axis of rotation. 52 Two primary arthrokinematic movements (rotation and anterior translation) occur at this joint around three planes: sagittal, horizontal, and frontal. Rotation occurs from the beginning to the midrange of movement. In addition to the rotational motions during mouth opening and closing and lateral deviations, movements at the TMJ involve arthrokinematic rolls and slides. Gliding, translation, or sliding movements occur in the upper cavity, whereas rotation or hinged movement occurs in the lower cavity. The motions of protrusion and retrusion are planar glides. Thus, mouth opening, contralateral deviation, and protrusion all involve an anterior osteokinematic rotation of the mandible and an anterior, inferior, and lateral glide of the mandibular head and disk; mouth closing, ipsilateral deviation, and retrusion all involve a posterior osteokinematic rotation of the mandible and an anterior, inferior, and lateral glide of the mandibular head and disk. Occlusal Position
Occlusal positions are functional positions of the TMJ. The occlusal position is defined as the point at which contact between some or all of the teeth occurs. Under normal circumstances, the upper molars rest directly on the lower molars and the upper incisors slightly override the lower incisors. The ideal position provides mutual protection of the anterior and posterior teeth, comfortable and painless mandibular function, and stability. 17 The median occlusal position corresponds to the position in which all of the teeth are fully interdigitated 19 and is considered the start position for all mandibular motions. The median occlusal position is dependent on the presence, shape, and position of the teeth. Protrusion of the upper or lower incisors, failure of the upper incisors to overlap with the lower incisors, absent or abnormally shaped teeth, and back teeth that do not meet are all causes of malocclusion. The centric position is considered to be the position that implies the most retruded, unstrained position of the mandible from which lateral movements are possible, and the components of the oral apparatus are the most balanced. 53 Ideally, the centric position should coincide with the median occlusal position. 53 It is worth remembering that malocclusion is probably very common in the general nonsymptomatic patient and may or may not be relevant to the presenting symptoms. 54 Rather than being a primary etiologic factor in TMD, malocclusion is likely to have a secondary or contributory role. 17 , 55 Mouth Opening
Mouth opening occurs in a series of steps ( Table 26-3 ). In the erect position, the condyles begin to rotate anteriorly and translate inferiorly and laterally during the first 25 degrees of opening as the jaw opens. The upper head of the lateral pterygoid muscle and the anterior head of the digastric muscle draw the disk anteriorly and prepare for condylar rotation during movement. 32 This initial condylar rotation occurs as the mandibular elevators (masseter, temporalis, and medial pterygoid muscles) gradually relax and lengthen, allowing gravity to depress the mandible (see Fig. 26-8 ). 32 The directions of the fibers of the lateral and medial temporomandibular ligaments also keep the condyle from moving posteriorly. The fibrous capsule and parts of the temporomandibular ligament limit excessive lateral movement of the condyle. The rotation occurs through the two condylar heads between the articular disk and the condyle. As the mandible moves forward on opening, the disks move medially and posteriorly until the collateral ligaments, and the lateral pterygoid stop their movement. During the last 15 degrees of opening, the rotation ceases due to tightening of the collateral ligaments, and is replaced by an anterior translation of the condyles (see Fig. 26-8 ). 56 During this translation, the condyle and disk move together. The anterior translation, which is produced mainly by muscle contraction, serves to prevent mandibular encroachment of the anterior neck structures. Opening is also assisted by the other suprahyoid muscles. 32 In extremely wide opening, such as that occurs with yawning, the functional joint contact is on the distal aspect of the condyle, and the anterior lateral aspect of the condyle contacts the posterior part of the masseter muscle. In this position, the soft-tissue structures are in a position of stretch, making them more prone to dysfunction. 57 FIGURE 26-8 Mouth opening and closing. TABLE 26-3 Arthrokinematic Steps of the Temporomandibular Joint Step Movement Rest position Joint is in an open-packed position Rotation There is a mid-opening Condylar joint surfaces glide forward, inferior joint surface of disk has a relative posterior glide, upper lateral pterygoid relaxes, inferior pterygoid contracts, and posterior connective tissue is in a functional state of rest Functional opening Disk and condyle experience a short anterior translatory glide; superior and inferior heads of lateral pterygoid contract to guide disk and condyle forward Posterior connective tissue is in a functional tightening Translation There is full opening Disk and condyle glide anteriorly and caudally Superior and inferior heads of lateral pterygoid contract to guide disk and condyle fully forward Posterior connective tissues tighten Closure Surface of condyle joint glides posteriorly, and disk glides relative to anterior surface Superior head of lateral pterygoid contracts and inferior head relaxes Posterior connective tissue returns to its functional length Data from Rocabado M. Arthrokinematics of the temporomandibular joint. In: Gelb H, ed. Clinical Management of Head, Neck and TMJ Pain and Dysfunction. Philadelphia, PA: WB Saunders; 1985. Mouth Closing
Closing of the mouth involves a reversal of the movements described for mouth opening. The condyles translate posteriorly as a result of an interaction between the retracting portions of the masseter and temporalis muscle and the retracting portions of the mandibular depressors (see Fig. 26-8 ). 52 As the condyles translate posteriorly and glide medially, they hinge on the disks. The disks then glide posteriorly and superiorly on the temporal bone along with the condyles (as a result of the actions of the masseter, medial pterygoid, and temporalis muscles). 42 When the jaws are closed to maximal occlusal contact, the condyles contact the disks, and the disks contact the posterior slopes of the articular tubercles and the glenoid fossae. Protrusion
Protrusion is a forward movement of the mandible that occurs at the superior joint compartments, which consists of the disk and condyle moving downward, forward, and laterally. The muscles responsible for protrusion are the anterior fibers of the temporalis and the medial and lateral pterygoid muscles. Retrusion
Retrusion is a backward movement of the mandible, produced by the posterior fibers of the temporalis and assisted by the suprahyoid muscles. The retrusive range is limited by the extensibility of the temporomandibular ligaments. 58 Lateral Excursion
If a protrusion movement occurs unilaterally, it is called a lateral excursion, or deviation. For example, if only the left TMJ protrudes, the jaw deviates to the right. Lateral movements of the mandible are the result of asymmetric muscle contractions ( Fig. 26-9 ). During a lateral excursion to the right, the condyle and the disk on the left side glide inferiorly, anteriorly, and laterally in the sagittal plane and medially in the horizontal plane along the articular eminence. The condyle and the disk on the right side rotate laterally on a sagittal plane and translate medially in the horizontal plane while remaining in the fossa. FIGURE 26-9 Lateral deviation to the left. CLINICAL PEARL The translation of the human condyle during jaw opening and lateral jaw movements is referred to as the Bennett shift. The Close- and Open-Packed (Resting) Positions
The close-packed position of the TMJ is difficult to determine because the position of maximal muscle tightness is also the position of least joint surface congruity and vice versa. Rocabado 56 considers there to be two close-packed positions, named according to the end position of the mandibular head in the fossa: Anterior close-packed position. This position is the position of maximum opening of the joint. Posterior close-packed position. This position is the maximum retruded position of the joint. Under this premise, the open-packed, or “rest” position is any position away from the anterior or posterior close-packed positions of the joint. 56 The rest position, or “freeway space” corresponds to the position of the TMJ where the residual tension of the muscles is at rest and no contact occurs between maxillary and mandibular teeth. In this position, the tongue is against the palate of the mouth with its most anterior–superior tip in the area just posterior to the rear of the upper central incisors. 59 Capsular Pattern
The capsular pattern of the TMJ is a limitation of mouth opening. If one joint is more involved than the other, the jaw will laterally deviate to the same side during opening. CLINICAL PEARL The significance of the rest position is that it permits the tissues of the stomatognathic system to rest and undergo repair. 60 EXAMINATION Currently, clinical examination is the gold standard for diagnosing TMDs. Given the multifactorial causes of TMD, a comprehensive examination of the entire upper quadrant, including the cervical spine and shoulders, usually is warranted. In general, the TMJ and the upper three cervical joints all refer symptoms to the head, whereas the mid-to-low cervical spine typically refers symptoms to the shoulder and the arm. 61–63 An accurate diagnosis of TMD involves a careful evaluation of the information gleaned from the history, systems review, and tests and measures. In most chronic cases, a behavioral or psychological examination is required. 3 , 31 , 63–68 Since postural dysfunctions are closely related to TMJ symptoms, the clinician should always perform a postural examination as part of a comprehensive examination of this joint. An examination form for the TMJ examination is shown in Table 26-4 . TABLE 26-4 Temporomandibular Examination Form History
A comprehensive history will help identify the possible source(s) of the orofacial pain and provide a screen for other causative or contributing factors. 69 During the history, the clinician should observe whether the patient’s mouth moves comfortably. The severity of the symptoms and the time before the symptoms subside can provide the clinician with valuable information regarding possible pathology. Red flags related to cardiac history (e.g., angina or history of myocardial infarction) and brain function (e.g., sudden-onset severe headaches, weakness, or slurred speech) must be investigated early in the history taking. 70 The clinician should determine from the patient the main reason for the visit. There are three cardinal features of TMDs, which can be local or remote: Restricted jaw function. Limited mouth opening, which may be reported as intermittent or progressive, is a key feature of TMD. A key question to determine restricted jaw function is, “Have you ever had your jaw lock or catch so that it would not open all the way? If so, was this limitation in jaw opening severe enough to interfere with your ability to eat? Have you ever noticed clicking, or popping or other sounds in your joint?” 71 Patients may describe a generalized tight feeling, which may indicate a muscular disorder, or capsulitis, or the sensation that the jaw suddenly “catches” or “locks,” which usually is related to a mechanical interference within the joint (an internal derangement). 16 Associated signs of an internal derangement include pain and deviation of mandibular movements during opening and closing (refer to Practice Pattern 4D, under “Intervention Strategies” section later), and biting firm objects. Pain in the fully open position is probably caused by an extra-articular problem. Locking may imply that the mouth does not fully open or does not fully close and is often related to problems of the disk or joint degeneration. A gradual onset of symptoms after minor or prolonged physical activity may be indicative of a mechanical derangement. Symptoms of a mechanical nature generally are eased with rest. The irritability of a disorder is determined by the degree of activity necessary to provoke a symptom response. Joint noises. Joint noises (crepitus) of the TMJ may or may not be significant, because joint sounds occur in approximately 50% of healthy populations. 72 Some joint sounds are not audible to the clinician, so a stethoscope may be required. “Hard” crepitus is a diffuse sustained noise that occurs during a significant portion of the opening or closing cycle, or both and is an evidence of a change in osseous contour. 57 Clicking describes a brief noise that occurs at some point during opening, closing, or both [see the discussion of range of motion (ROM) testing, later]. Jaw clicking during mouth opening or closing may be suggestive of an internal derangement consisting of an anterior disk displacement with reduction. 73 , 74 Orofacial pain. TMJ pain should be evaluated carefully in terms of its onset, nature, intensity, site, duration, aggravating and relieving factors, and how it relates to joint noise and restricted mandibular movements. Information about the nature of the pain will be critical in determining the possibility of primary headaches (migraine, cluster) and secondary headaches related to the eyes, ears, sinus, dental structures, medication complications, and/or neurologic types of pain. Unrelenting pain unrelated to musculoskeltal function is an indication for referral. Key questions have been examined and determined to have strong sensitivity and specificity in incriminating TMDs as the source of pain. 76 The initiating question should be, “Have you had pain or stiffness in the face, jaw, temple, in front of the ear, or in the ear in the past month?” 70 A positive response should be followed by a question about whether the symptoms are altered by any of the following jaw activities: chewing, talking, singing, yawning, kissing, moving the jaw. 69 Specific questions about activities and postures of a sustained nature, such as sitting, sleeping, and driving, should be asked. Orofacial pain associated with mouth opening or closing and jaw crepitus is suggestive of osteoarthrosis, capsulitis, or internal derangement consisting of an anterior disk displacement with reduction. 73 , 74 Information about cervical dysfunction is essential to determine whether the cervical spine is causing or exacerbating the headache/facial pain. 70 In a study by Magnusson et al., 77 five different scales of self-assessment of pain were tested in patients with TMJ disorders. The precision and sensitivity and the capacity to register memory of pain and discomfort were compared for each of the five scales ( Table 26-5 ). From these results, the behavior rating scale can be recommended when measuring pain and discomfort in patients with TMJ disorders. TABLE 26-5 Patient Reports of Pain in TMJ Disorders Test and Measure Test Procedure Population Reliability Kappa Values Visual analog scale 100-mm line with the end defined as no pain and worst pain imaginable 38 consecutive patients referred with TMJ disorders κ = 0.38 Numeric scale 10-point scale with 0 indicating no paint and 10 representing worst pain κ = 0.36 Behavior rating scale Six-point scale ranging from minor discomfort to very strong discomfort κ = 0.68 Verbal scale Five-point scale ranging from no pain to very severe pain κ = 0.44 Data from Magnusson T, List T, Helkimo M. Self-assessment of pain and discomfort in patients with temporomandibular disorders: a comparison of five different scales with respect to their precision and sensitivity as well as their capacity to register memory of pain and discomfort. J Oral Rehabil. 1995;22:549–556.; Cleland J. Temporomandibular Joint, Orthopaedic Clinical Examination: An Evidence-Based Approach for Physical Therapists . Carlstadt, NJ. Icon Learning Systems, LLC; 2005:39–89. With permission from Icon Learning Systems. In addition, it is important to determine: If the presenting symptoms were caused by trauma or surgery, or if the onset of pain occurred gradually. Questions should focus on any history of trauma during birth or childhood, as well as more recently. If there are any emotional factors in the patient’s background that may provoke habitual protrusion or muscular tension. Chronic head, neck, and back pain often are associated with psychogenic causes. Psychiatric disorders, usually, are manifested in patients whose afflictions seem to be excessive or persist beyond what would be normal for that condition. The clinician should listen for reports of psychological stress overload, malaise, anxiety, sleep problems, changes in eating patents, weight changes, unexplained fatigue, and other signs of depression, which might exacerbate pain through central mechanisms. 79 The checklist outlined in Table 26-6 can be used by the clinician to identify factors that may warrant an examination by a mental health professional. TABLE 26-6 Checklist of Psychological and Behavioral Factors Inconsistent, inappropriate, or vague reports of pain Overdramatization of symptoms Symptoms that vary with life events Significant pain of >6 months’ duration Repeated failures with conventional therapies Inconsistent response to medications History of other stress-related disorders Major life events (e.g., new job, marriage, divorce, and death) Evidence of drug abuse Clinically significant anxiety or depression Evidence of secondary gain Note: The significance of these factors depends on the particular patient. Data from McNeill C, Mohl ND, Rugh JD, et al. Temporomandibular disorders: Diagnosis, management, education, and research. J Am Dent Assoc. 1990;120:253–260. If the patient is aware of any parafunctional habits (cheek biting, nail biting, pencil chewing, teeth clenching, or bruxism). For example, does the patient chew on one side more than the other? Chewing more on one side versus the other is typically the result of malocclusion (see later). In addition, favoring one side can lead to a loss of vertical dimension (the distance between any two arbitrary points on the face). A simple way to measure the aforementioned is to measure from the lateral edge of the eye to the corner of the mouth and from the base of the nose to the chin. The behavior of symptoms over a 24-hour period. This information assists the clinician in formulating causal relationships. Whether the symptoms are improving or worsening. The relationship of eating to the symptoms. Alcohol, chocolate, and other foods such as ice cream can cause head pain in some individuals, suggesting a vasomotor-related pain. The patient’s past dental and orthodontic history. CLINICAL PEARL TMJ sounds should be described and related to symptoms. Joint noise is, of itself, of little clinical importance in the absence of pain. 65 , 75
CLINICAL PEARL Pain that is centered immediately in front of the tragus of the ear and that projects to the ear, temple, cheek, and along the mandible is highly diagnostic for TMD. 78 Systems Review
Pain or dysfunction in the orofacial region often results from nonmusculoskeletal causes such as otolaryngologic, neurologic, vascular, neoplastic, psychogenic, and infectious diseases. Clinicians often see patients with a TMD who present with nonspecific symptoms such as neck pain, headaches (see Chapter 5 ), earaches, tinnitus, and sinusitis. 70 Patients with sinusitis complain of acute facial pain or pressure type headaches, and may present with nasal congestion, a reduced sense of smell, postnasal drip, fever or malaise, and aching teeth associated with certain weather conditions or times of the year. 80 Ear disorders, such as an inner or outer ear infection, can produce pre-auricular symptoms in around the TMJ. 81 Conversely, hyperactivity of the masticatory and tensor tympani muscles can cause ear pain, tinnitus, and feelings of fullness in the ear. 82 Finally, patients with eye disorders may experience pain around the eye, numbness, a headache, and other symptoms similar to TMD, a cervicogenic headache (see Chapter 23 ), or a primary headache (see Chapter 5 ). 70 Unexplained weight loss, ataxia, weakness, fever with pain, nystagmus, and neurologic deficits are characteristic of intracranial disorders. 83 Neurovascular disorders are associated with a migraine headache and its variants, carotidynia, and cluster headaches (see Chapter 5 ). Neuropathic disorders include trigeminal neuralgia, glossopharyngeal neuralgia, and occipital neuralgia. A cranial nerve screen (see Chapter 3 ) should be completed on each patient presenting with orofacial pain with particular attention on the fifth cranial nerve (trigeminal), which supplies motor and sensory innervation to the masticatory region. Once the possibility of cervical, systemic, psychogenic, or ear or sinus problems has been ruled out, the next step is to consider the possibility of TMJ pain and impairment. Tests and Measures
Examination of the TMJ structures includes observation, and a thorough mobility and palpation examination to identify impairments and functional limitations. Observation
The posture of the head and neck are assessed for asymmetry. The forward head posture (FHP–see Chapters 6 and 25 ) frequently is associated with TMD. 34 , 84 , 85 This is likely because of the direct impact an FHP can have on oral symmetry during occlusion. Occlusion occurs when the teeth are in contact and the mouth is closed—when tapping the teeth together in the neutral position, all of the teeth appear to strike simultaneously. However, if the same task is attempted while placing the head forward, it is the anterior teeth that occlude first. A deviation from normal occlusion is defined as malocclusion—improper positioning of the teeth and jaws. Malocclusion is a variation of normal growth and development which can affect the bite, the ability to clean teeth properly, gum tissue health, jaw growth, speech development, and appearance. The consequences of this repetitive functional malocclusion during food or gum chewing should be apparent. A chronic FHP may result in an adaptive shortening of the deep cervical fascia and muscles, which can exaggerate the functional malocclusion. Most people have some degree of malocclusion, although it is not usually serious enough to require treatment. Malocclusions can be divided mainly into three types, depending on the sagittal relations of teeth and jaws, by Angle’s classification method, which is based on the relative position of the first maxillary molar 86 : Class I (Neutroclusion): The molar relationship of the occlusion is normal, but the other teeth have problems such as spacing, crowding, and over or under eruption. Class II (Distoclusion): The upper molars are placed anteriorly. There are two subtypes: Class II Division 1 (large overjet): The molar relationships are like that of Class II and the anterior teeth are protruded. Class II Division 2 (deep overbite): The molar relationships are like that of class II but there is lateral flaring of the lateral maxillary incisors. Class III (Mesioclusions): The lower front teeth are more prominent than the upper front teeth. In this case, the patient very often has a large mandible or a short maxillary bone. The clinician should also note whether the teeth are normally aligned or whether there is any crossbite, underbite, or overbite. Crossbite: This occurs when the teeth of the mandible are lateral to the upper maxillary teeth on one side and medial on the opposite side. An anterior crossbite occurs when the lower incisors are anterior to the upper incisors, whereas a posterior crossbite occurs when there is a abnormal transverse relationship of the teeth. Underbite: This occurs when the mandibular teeth are anterior to the maxillary teeth either unilaterally, bilaterally, or in pairs. Overbite: This occurs when the anterior maxillary incisors extend below the anterior mandibular incisors when the jaw is in central occlusion.
Share this:
- Click to share on Twitter (Opens in new window)
- Click to share on Facebook (Opens in new window)
Related posts:

Stay updated, free articles. Join our Telegram channel
Comments are closed for this page.

Full access? Get Clinical Tree

COMMENTS
Protrusion, retrusion, and excursion demonstrated with free video, pictures, and anatomy review quiz. Learn anatomy body movement terms for your anatomy and physiology courses in nursing school and other healthcare majors.
Excursion Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Excursion Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Excursion Excursion is the side-to-side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Flexion and extension are typically movements that take place within the sagittal plane and involve anterior or posterior movements of the neck, trunk, ...
Excursion Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Protrusion, retrusion, and excursion are terms used in anatomy to describe body movements going anteriorly (forward), posteriorly (backward), or side-to-side...
In this anatomy lesson, I'm going to demonstrate protrusion, retrusion, and excursion, which are special body movement terms in anatomy that refer to forward (anterior), backward (posterior), or side to side movements.
Dynamic occlusion: lateral excursion The dynamic occlusion is the contact that teeth make during movements of the mandible - when the jaw moves side to side, forward, backward or at an angle.
Excursion Excursion is the side to side movement of the mandible. Lateral excursion moves the mandible away from the midline, toward either the right or left side. Medial excursion returns the mandible to its resting position at the midline.
Anatomical terms of movement are used to describe the actions of muscles upon the skeleton. Muscles contract to produce movement at joints, and the subsequent movements can be precisely described using this terminology.
Simply put, lateral excursion is when the mandible moves to one side. But the mechanism behind this is not as simple as it sounds. The mandible is capable of two movements if we take the condyle as the hinge: rotation and translation. Imagine a vertical and horizontal axis passing through the condyles. The movement of the mandible with respect ...
TMJ Movements. Normal movements of the jaw during function, such as chewing, are known as excursions. There are two lateral excursions ( left and right ) and the forward excursion, known as protrusion, the reversal of which is retrusion. When the jaw is moved into protrusion, the lower incisors or front teeth are moved so that they first come ...
During a lateral excursion to the right, the condyle and the disk on the left side glide inferiorly, anteriorly, and laterally in the sagittal plane and medially in the horizontal plane along the articular eminence.
lateral excursion: [ ek-skur´zhun ] a range of movement regularly repeated in performance of a function, e.g., excursion of the jaws in mastication. adj., adj excur´sive. lateral excursion sideward movement of the mandible between the position of closure and the position in which cusps of opposing teeth are in vertical proximity.
Answer Q. Discuss the joints involved and movements required for you to cross your arms together in front of your chest. Answer Glossary abduction adduction circumduction depression dorsiflexion elevation eversion extension flexion hyperextension hyperflexion inferior rotation inversion lateral excursion lateral flexion lateral (external ...
excursion. [ ek-skur´zhun] a range of movement regularly repeated in performance of a function, e.g., excursion of the jaws in mastication. adj., adj excur´sive. lateral excursion sideward movement of the mandible between the position of closure and the position in which cusps of opposing teeth are in vertical proximity.